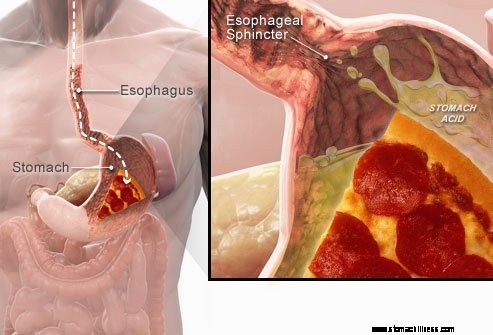
 Kun nielet ruokaa, se kulkee ruokatorvea pitkin alas ruokatorven sulkijalihaksena tunnetun lihasrenkaan läpi ( LES). Tämä rakenne avautuu, jotta ruoka pääsee vatsaan. Sen on tarkoitus pysyä suljettuna, jotta mahalaukun sisältö pysyy paikallaan.
Kun nielet ruokaa, se kulkee ruokatorvea pitkin alas ruokatorven sulkijalihaksena tunnetun lihasrenkaan läpi ( LES). Tämä rakenne avautuu, jotta ruoka pääsee vatsaan. Sen on tarkoitus pysyä suljettuna, jotta mahalaukun sisältö pysyy paikallaan.
GERD eli happamat refluksioireet johtuvat happaman nestemäisen mahalaukun sisällön takaisinvirtauksesta ruokatorveen. Yleisin GERD:n oire on närästys.
Muita oireita, joita voi ilmetä GERD:n seurauksena, ovat:
 Yleisin GERD:n oire on närästys.
Yleisin GERD:n oire on närästys. Gastroesofageaalinen refluksitauti, jota yleisesti kutsutaan GERD:ksi tai happorefluksiksi, on tila, jossa mahalaukun nestesisältö regurgitoituu (palautuu tai palautuu) ruokatorveen. Neste voi tulehduttaa ja vahingoittaa limakalvoa (esofagiitti), vaikka näkyviä tulehduksen merkkejä esiintyy vähemmistöllä potilaista. Rukoileva neste sisältää yleensä mahalaukun tuottamaa happoa ja pepsiiniä. (Pepsiini on entsyymi, joka aloittaa proteiinien sulamisen mahassa.) Palautettu neste voi myös sisältää sappia, joka on palautunut mahalaukkuun pohjukaissuolesta. Ensimmäinen ohutsuolen osa kiinnittyy vatsaan. Hapon uskotaan olevan palautusjäähdytetyn nesteen vahingollisin komponentti. Pepsiini ja sappi voivat myös vahingoittaa ruokatorvea, mutta niiden rooli ruokatorven tulehduksen ja vaurion tuottamisessa ei ole yhtä selvä kuin hapon rooli.
GERD on krooninen sairaus. Kun se alkaa, se on yleensä elinikäinen. Jos ruokatorven limakalvossa on vaurio (esofagiitti), tämä on myös krooninen tila. Lisäksi, kun ruokatorvi on parantunut hoidolla ja hoito on lopetettu, vamma palaa useimmilla potilailla muutaman kuukauden kuluessa. Kun GERD:n hoito on aloitettu, sitä on jatkettava toistaiseksi. Joitakin potilaita, joilla on ajoittaisia oireita ja joilla ei ole ruokatorvitulehdusta, voidaan kuitenkin hoitaa vain oireiden aikana.
Itse asiassa mahalaukun nestemäisen sisällön palautuminen ruokatorveen tapahtuu useimmilla normaaleilla yksilöillä. Eräässä tutkimuksessa havaittiin, että refluksia esiintyy usein normaaleilla yksilöillä kuten potilailla, joilla on GERD. GERD-potilailla refluksoitu neste sisältää kuitenkin useammin happoa ja happo pysyy ruokatorvessa pidempään. On myös havaittu, että neste palautuu ruokatorveen korkeammalle tasolle GERD-potilailla kuin tavallisilla henkilöillä.
Kuten usein tapahtuu, keholla on keinoja suojautua refluksin ja hapon haitallisilta vaikutuksilta. Esimerkiksi useimmat refluksitautia esiintyy päivän aikana, kun ihmiset ovat pystyasennossa. Pystyasennossa palautusjäähdytetty neste virtaa todennäköisemmin takaisin vatsaan painovoiman vaikutuksesta. Lisäksi, kun ihmiset ovat hereillä, he nielevät toistuvasti riippumatta siitä, onko refluksia tai ei. Jokainen nielee kaiken palautusjäähdytetyn nesteen takaisin mahalaukkuun. Lopuksi suun sylkirauhaset tuottavat sylkeä, joka sisältää bikarbonaattia. Jokaisen nielemisen yhteydessä bikarbonaattia sisältävä sylki kulkee ruokatorvea pitkin. Bikarbonaatti neutraloi pienen määrän happoa, joka jää ruokatorveen sen jälkeen, kun painovoima ja nieleminen on poistanut suurimman osan happamasta nesteestä.
Painovoima, nieleminen ja sylki ovat tärkeitä ruokatorven suojamekanismeja, mutta ne ovat tehokkaita vain, kun henkilöt ovat pystyasennossa. Yöllä unen aikana painovoimalla ei ole vaikutusta, nieleminen lakkaa ja syljen eritys vähenee. Siksi yöllä esiintyvä refluksi johtaa todennäköisemmin siihen, että happo pysyy ruokatorvessa pidempään ja aiheuttaa suurempaa vahinkoa ruokatorvelle.
Tietyt olosuhteet tekevät henkilön alttiiksi GERD:lle. Esimerkiksi GERD voi olla vakava ongelma raskauden aikana. Raskauden kohonneet hormonitasot aiheuttavat todennäköisesti refluksia alentamalla ruokatorven alasulkijalihaksen painetta (katso alla). Samaan aikaan kasvava sikiö lisää painetta vatsassa. Molempien näiden vaikutusten odotetaan lisäävän refluksia. Myös potilaat, joilla on ruokatorven lihaksia heikentäviä sairauksia, kuten skleroderma tai sekamuotoiset sidekudossairaudet, ovat alttiimpia GERD:lle.
GERD:n syy on monimutkainen ja siihen voi liittyä useita syitä. Lisäksi eri syyt voivat vaikuttaa eri yksilöihin tai jopa samaan yksilöön eri aikoina. Pieni määrä GERD-potilaita tuottaa epätavallisen suuria määriä happoa, mutta tämä on harvinaista, eikä se vaikuta suurimmalla osalla potilaista.
GERD:hen vaikuttavat tekijät ovat:
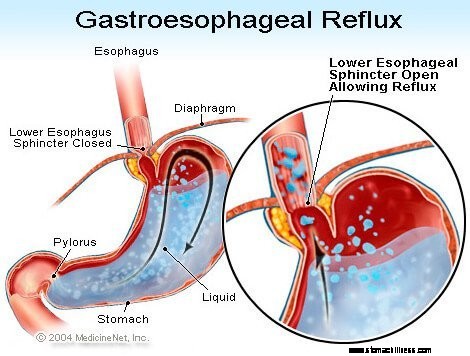
Ruokatorven alemman sulkijalihaksen (LES) toiminta on ehkä tärkein tekijä (mekanismi) refluksin estämisessä. Ruokatorvi on lihaksikas putki, joka ulottuu kurkun alaosasta mahalaukkuun. LES on erikoistunut lihasrengas, joka ympäröi ruokatorven alinta päätä, jossa se liittyy mahalaukkuun. LES:n muodostava lihas on aktiivinen suurimman osan ajasta, eli levossa. Tämä tarkoittaa, että se supistuu ja sulkee kulkua ruokatorvesta mahalaukkuun. Tämä käytävän sulkeminen estää refluksoinnin. Kun ruokaa tai sylkeä niellään, LES rentoutuu muutaman sekunnin ajan, jotta ruoka tai sylki pääsee kulkeutumaan ruokatorvesta mahalaukkuun, ja sitten se sulkeutuu uudelleen.
Useita erilaisia LES:n poikkeavuuksia on havaittu potilailla, joilla on GERD. Kaksi niistä koskee LES:n toimintaa. Ensimmäinen on LES:n epänormaalin heikko supistuminen, mikä vähentää sen kykyä estää refluksi. Toinen on LES:n epänormaalit relaksaatiot, joita kutsutaan ohimeneviksi LES-relaksaatioiksi. Ne ovat epänormaaleja siinä mielessä, että ne eivät ole nielemisen mukana ja kestävät pitkään, jopa useita minuutteja. Nämä pitkittyneet rentoutukset mahdollistavat refluksin esiintymisen helpommin. Ohimeneviä LES-relaksaatioita esiintyy GERD-potilailla yleisimmin aterioiden jälkeen, kun vatsa on turvonnut ruoan kanssa. Ohimeneviä LES-relaksaatioita esiintyy myös henkilöillä, joilla ei ole GERD:tä, mutta ne ovat harvinaisia.
Viimeisin GERD-potilailla kuvattu poikkeavuus on LES:n löysyys. Erityisesti samanlaiset venymispaineet avaavat LES:n enemmän potilailla, joilla on GERD kuin henkilöillä, joilla ei ole GERD:tä. Ainakin teoriassa tämä mahdollistaisi LES:n helpomman avaamisen ja/tai suuremman hapon virtauksen taaksepäin ruokatorveen, kun LES on auki.
Hiatal-tyrät edistävät refluksia, vaikka tapa, jolla ne vaikuttavat, ei ole selvää. Suurimmalla osalla GERD-potilaista on hiatal-tyrä, mutta monilla ei. Siksi GERD:n saamiseksi ei tarvitse olla hiatal-tyrää. Lisäksi monilla ihmisillä on hiatal-tyrä, mutta heillä ei ole GERD:tä. Ei tiedetä varmasti, miten tai miksi hiataltyrät kehittyvät.
Normaalisti LES sijaitsee samalla tasolla, jossa ruokatorvi kulkee rinnasta pallean pienen aukon kautta vatsaan. (Pallea on lihaksikas, vaakasuora väliseinä, joka erottaa rinnan vatsasta.) Kun on hiataltyrä, pieni osa ruokatorveen kiinnittyvää ylävatsaa työntyy ylös pallean läpi. Tämän seurauksena pieni osa vatsasta ja LES:stä asettuvat rintaan, eikä LES ole enää pallean tasolla.
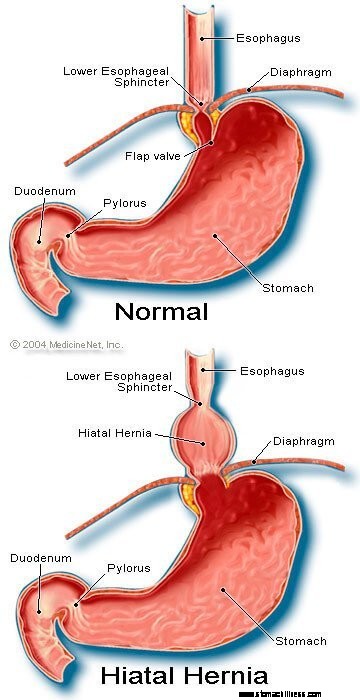 Kuva hiatal-tyrästä
Kuva hiatal-tyrästä
Vaikuttaa siltä, että LES:tä ympäröivä kalvo on tärkeä refluksin estämisessä. Toisin sanoen henkilöillä, joilla ei ole hiatal-tyrää, ruokatorvea ympäröivä pallea supistuu jatkuvasti, mutta sitten rentoutuu nieltäessä, aivan kuten LES. Huomaa, että LES:n ja pallean vaikutukset esiintyvät samassa paikassa potilailla, joilla ei ole hiatal-tyrää. Siksi refluksoinnin este on yhtä suuri kuin LES:n ja kalvon synnyttämien paineiden summa. Kun LES siirtyy rintaan, jossa on hiatal-tyrä, pallea ja LES jatkavat paineensa ja estevaikutuksensa kohdistamista. Nyt he tekevät niin kuitenkin eri paikoissa. Näin ollen paineet eivät ole enää additiivisia. Sen sijaan yksi korkeapaineinen refluksoinnin esto korvataan kahdella alhaisemman paineen esteellä, jolloin palautusvirtaus tapahtuu helpommin. Joten paineesteen alentaminen on yksi tapa, jolla hiataltyrä voi edistää refluksia.
Kuten aiemmin mainittiin, nielet ovat tärkeitä hapon poistamisessa ruokatorvesta. Nieleminen aiheuttaa ruokatorven lihasten rengasmaisen supistumisaallon, joka kaventaa ruokatorven onteloa (sisäonteloa). Supistuminen, jota kutsutaan peristaltiksi, alkaa ruokatorven yläosasta ja kulkee ruokatorven alaosaan. Se työntää ruokaa, sylkeä ja kaikkea muuta ruokatorvessa olevaa vatsaan.
Kun supistumisaalto on viallinen, refluksoitua happoa ei työnnetä takaisin mahalaukkuun. GERD-potilailla on kuvattu useita supistuksen poikkeavuuksia. Esimerkiksi supistumisaallot eivät välttämättä ala jokaisen nielemisen jälkeen tai supistumisaallot voivat kuolla pois ennen kuin ne saavuttavat mahalaukun. Myös supistusten synnyttämä paine voi olla liian heikko työntämään happoa takaisin mahalaukkuun. Tällaisia supistuksen poikkeavuuksia, jotka vähentävät hapon puhdistumaa ruokatorvesta, havaitaan usein potilailla, joilla on GERD. Itse asiassa niitä esiintyy useimmiten niillä potilailla, joilla on vaikein GERD. Epänormaalien ruokatorven supistuksen vaikutusten odotetaan olevan pahempia yöllä, kun painovoima ei auta palauttamaan refluksoitua happoa mahalaukkuun. Huomaa, että tupakointi vähentää myös merkittävästi hapon puhdistumaa ruokatorvesta. Tämä vaikutus jatkuu vähintään 6 tuntia viimeisen savukkeen jälkeen.
Suurin osa reflukseista päivän aikana tapahtuu aterioiden jälkeen. Tämä refluksi johtuu todennäköisesti ohimenevistä LES-relaksaatioista, jotka johtuvat mahalaukun venymisestä ruoan kanssa. Pienellä osalla GERD-potilaista on havaittu mahalaukun, joka tyhjenee epätavallisen hitaasti aterian jälkeen. Tätä kutsutaan gastropareesiksi. Vatsan hitaampi tyhjeneminen pidentää mahalaukun turvotusta ruoan kanssa aterioiden jälkeen. Siksi hitaampi tyhjennys pidentää aikaa, jonka aikana refluksi on todennäköisempi. Mahalaukun tyhjentymisen heikkenemiseen liittyy useita lääkkeitä, kuten:
Henkilöiden ei tule lopettaa näiden tai muiden määrättyjen lääkkeiden käyttöä ennen kuin lääkkeen määräävä lääkäri on keskustellut heidän kanssaan mahdollisesta GERD-tilanteesta.
Komplisoitumattoman GERD:n oireet ovat ensisijaisesti:
Muita oireita esiintyy GERD:n komplikaatioiden yhteydessä, ja niistä keskustellaan komplikaatioiden kanssa.
Kun happo palautuu takaisin ruokatorveen GERD-potilailla, ruokatorven hermosäikeet stimuloituvat. Tämä hermostimulaatio johtaa useimmiten närästykseen, kipuun, joka on tyypillistä GERD:lle. Närästystä kuvataan yleensä polttavaksi kivuksi rintakehän keskellä. Se voi alkaa korkealta vatsasta tai voi ulottua kaulaan. Joillakin potilailla kipu voi kuitenkin olla terävää tai painetta muistuttavaa, ei polttavaa. Tällainen kipu voi jäljitellä nivelkipua (angina). Muilla potilailla kipu voi ulottua selkään asti.
Koska happorefluksi on yleisempää aterioiden jälkeen, närästys on yleisempää aterioiden jälkeen. Närästys on yleisempää myös makuulla, koska ilman painovoiman vaikutuksia refluksi tapahtuu helpommin ja happo palautuu mahaan hitaammin. Monet GERD-potilaat herättävät unesta närästyksen.
Närästysjaksoilla on taipumus esiintyä ajoittain. Tämä tarkoittaa, että jaksot ovat yleisempiä tai vakavia useiden viikkojen tai kuukausien ajan ja muuttuvat sitten harvemmiksi tai vakaviksi tai jopa poissa useiden viikkojen tai kuukausien ajan. Tämä oireiden toistuvuus tarjoaa perusteen ajoittaiselle hoidolle GERD-potilailla, joilla ei ole esofagiittia. Närästys on kuitenkin elinikäinen ongelma, ja se palaa melkein aina.
Regurgitaatio on refluksoituneen nesteen esiintyminen suussa. Useimmilla GERD-potilailla ruokatorveen pääsee yleensä vain pieniä määriä nestettä, ja neste jää ruokatorven alaosaan. Toisinaan joillakin GERD-potilailla suuremmat nestemäärät, jotka joskus sisältävät ruokaa, refluksoidaan ja ne saavuttavat ruokatorven yläosan.
Ruokatorven yläpäässä on ylempi ruokatorven sulkijalihas (UES). UES on pyöreä lihasrengas, joka on toiminnaltaan hyvin samanlainen kuin LES. Toisin sanoen UES estää ruokatorven sisällön palautumisen kurkkuun. Kun pieniä määriä refluksoitua nestettä ja/tai ruokaa joutuu UES:n ohi ja joutuu kurkkuun, suussa saattaa olla hapan makua. Jos suuremmat määrät rikkovat UES:n, potilaat voivat yhtäkkiä löytää suunsa täynnä nestettä tai ruokaa. Lisäksi toistuva tai pitkittynyt regurgitaatio voi johtaa hapon aiheuttamiin hampaiden eroosioihin.
Pahoinvointi on harvinaista GERD:ssä. Joillakin potilailla se voi kuitenkin olla usein tai vaikeaa ja johtaa oksentamiseen. Itse asiassa potilailla, joilla on selittämätöntä pahoinvointia ja/tai oksentelua, GERD on yksi ensimmäisistä huomioon otettavaista sairauksista. Ei ole selvää, miksi joillekin GERD-potilaille kehittyy pääasiassa närästystä ja toisille pääasiassa pahoinvointia.
Neste vatsasta, joka palautuu ruokatorveen, vahingoittaa ruokatorven soluja. Keho reagoi samalla tavalla kuin se tavallisesti reagoi vaurioihin, jotka liittyvät tulehdukseen (esofagiitti). Tulehduksen tarkoituksena on neutraloida vaurioittava aine ja aloittaa paranemisprosessi. Jos vaurio menee syvälle ruokatorveen, muodostuu haavauma. Haava on yksinkertaisesti ruokatorven limakalvon katkeaminen, joka ilmenee tulehdusalueella. Haavaumat ja niiden aiheuttama lisätulehdus voivat syöpyä ruokatorven verisuoniin ja aiheuttaa verenvuotoa ruokatorveen.
Joskus verenvuoto on vakavaa ja saattaa vaatia:
Ruokatorven haavat paranevat muodostumalla arpia (fibroosia). Ajan myötä arpikudos kutistuu ja kaventaa ruokatorven onteloa (sisäonteloa). Tätä arpeutunutta kapenemista kutsutaan ahtaudeksi. Nielty ruoka voi juuttua ruokatorveen, kun kaventuminen on riittävän voimakasta (yleensä kun se rajoittaa ruokatorven ontelon halkaisijaltaan yhden sentin). Tämä tilanne voi edellyttää kiinnijääneen ruoan endoskooppista poistamista. Tämän jälkeen, jotta ruoka ei tarttuisi, kavennusta on venytettävä (levennettävä). Lisäksi refluksi on estettävä ahtauman toistumisen estämiseksi.
Pitkäaikainen ja/tai vaikea GERD aiheuttaa joillakin potilailla muutoksia ruokatorven soluissa. Nämä solut ovat syöpää esiasteita ja voivat, vaikkakin yleensä, muuttua syöpää aiheuttaviksi. Tätä tilaa kutsutaan Barrettin ruokatorveksi ja sitä esiintyy noin 10 %:lla GERD-potilaista. Barrettin ruokatorveen liittyvä ruokatorven syöpä (adenokarsinooma) yleistyy. Ei ole selvää, miksi joillekin GERD-potilaille kehittyy Barrettin ruokatorvi, mutta useimmat eivät.
Barrettin ruokatorvi voidaan tunnistaa visuaalisesti endoskopian yhteydessä ja vahvistaa limakalvosolujen mikroskooppisella tutkimuksella. Sitten Barrettin ruokatorvea sairastaville potilaille voidaan tehdä määräajoin seurantaendoskopia ja biopsia, vaikka ei ole yksimielisyyttä siitä, mitkä potilaat tarvitsevat seurantaa. Seurannan tarkoituksena on havaita eteneminen esisyövästä syöpää aiheuttavampiin muutoksiin, jotta syöpää ehkäisevä hoito voidaan aloittaa. Uskotaan myös, että Barrettin ruokatorvea sairastavien potilaiden tulisi saada maksimaalista GERD-hoitoa estämään ruokatorven lisävaurioita. Tutkitaan menetelmiä, joilla poistetaan epänormaalit limakalvosolut. Solujen poistamiseen voidaan käyttää useita endoskooppisia, ei-kirurgisia tekniikoita. Nämä tekniikat ovat houkuttelevia, koska ne eivät vaadi leikkausta; Niihin liittyy kuitenkin komplikaatioita, eikä hoitojen pitkäaikaista tehokkuutta ole vielä määritetty. Ruokatorven kirurginen poisto on aina vaihtoehto.
Monet hermot ovat ruokatorven alaosassa. Joitakin näistä hermoista stimuloi refluksoitu happo, ja tämä stimulaatio johtaa kipuun (yleensä närästykseen). Muut stimuloidut hermot eivät tuota kipua. Sen sijaan ne stimuloivat muita hermoja, jotka provosoivat yskää. Tällä tavalla refluksoitu neste voi aiheuttaa yskää ilman, että se koskaan ulottuu kurkkuun! Samalla tavalla refluksi alempaan ruokatorveen voi stimuloida ruokatorven hermoja, jotka liittyvät keuhkoihin ja voivat stimuloida hermoja, jotka menevät keuhkoihin. Nämä keuhkoihin menevät hermot voivat sitten aiheuttaa pienempien hengitysputkien kapenemisen, mikä johtaa astmakohtaukseen.
Vaikka GERD voi aiheuttaa yskää, se ei ole yleinen selittämättömän yskän syy. Vaikka GERD voi myös olla astman syy, on todennäköisempää, että se aiheuttaa astmakohtauksia potilailla, joilla on jo astma. Vaikka krooninen yskä ja astma ovat yleisiä vaivoja, ei ole selvää, kuinka usein GERD pahenee tai aiheuttaa niitä.
Jos refluksoitu neste pääsee ylemmän ruokatorven sulkijalihaksen ohi, se voi päästä kurkkuun (nieluun) ja jopa äänilaatikkoon (kurkunpää). Tuloksena oleva tulehdus voi aiheuttaa kurkkukipua ja käheyttä. Kuten yskimisen ja astman kohdalla, ei ole selvää, kuinka usein GERD on vastuussa muuten selittämättömästä kurkun ja kurkunpään tulehduksesta.
Refluksoitunut neste, joka kulkee kurkusta (nielu) ja kurkunpään sisään, voi päästä keuhkoihin (aspiraatio). Nesteen palautuminen keuhkoihin (kutsutaan aspiraatioksi) johtaa usein yskimiseen ja tukehtumiseen. Aspiraatiota voi kuitenkin esiintyä myös ilman näitä oireita. Näillä oireilla tai ilman niitä, aspiraatio voi johtaa keuhkoinfektioon ja johtaa keuhkokuumeeseen. Tämäntyyppinen keuhkokuume on vakava ongelma, joka vaatii välitöntä hoitoa. Kun aspiraatioon ei liity oireita, se voi johtaa keuhkojen hitaaseen, etenevään arpeutumiseen (keuhkofibroosi), joka voidaan nähdä rintakehän röntgenkuvissa. Aspiraatiota esiintyy todennäköisemmin yöllä, koska silloin refluksia vastaan suojaavat prosessit (mekanismit) eivät ole aktiivisia ja keuhkoja suojaava yskimisrefleksi ei myöskään ole aktiivinen.
Kurkku kommunikoi nenäkäytävien kanssa. Pienillä lapsilla kaksi imusolmuketta, joita kutsutaan adenoideiksi, sijaitsevat siellä, missä kurkun yläosa liittyy nenäkäytävään. Poskionteloiden kanavat ja keskikorvan putket (Eustachian putket) avautuvat nenäkäytävien takaosaan lähellä adenoideja. Refluksoitunut neste, joka pääsee ylempään kurkkuun, voi tulehduttaa adenoideja ja aiheuttaa niiden turpoamisen. Turvonneet adenoidit voivat sitten tukkia kanavat poskionteloista ja Eustachian putkista. Kun poskiontelot ja välikorvat sulkeutuvat nenäkäytävästä adenoidien turvotuksen vuoksi, niihin kerääntyy nestettä. Tämä nesteen kerääntyminen voi aiheuttaa epämukavuutta poskionteloissa ja korvissa. Koska adenoidit ovat näkyvissä pienillä lapsilla, eivät aikuisilla, tämä nesteen kerääntyminen korviin ja poskionteloihin on havaittavissa lapsilla, ei aikuisilla.
On olemassa erilaisia toimenpiteitä, testejä ja oireiden (esimerkiksi närästyksen) arviointia GERD-potilaiden diagnosoimiseksi ja arvioimiseksi.
Tavallinen tapa, että GERD on ominaisen oireensa perusteella, närästys. Närästystä kuvataan useimmiten rintalastan alapuolella (rintakehän keskiosan alla) poltettavaksi, joka ilmenee aterioiden jälkeen ja pahenee usein makuulla. Diagnoosin vahvistamiseksi lääkärit usein hoitavat potilaita lääkkeillä, jotka estävät mahalaukun hapon tuotantoa. Jos närästys on sitten vähentynyt suuressa määrin, GERD-diagnoosi katsotaan vahvistetuksi. Tätä lähestymistapaa, jossa diagnoosi tehdään oireiden hoitovasteen perusteella, kutsutaan yleisesti terapeuttiseksi kokeeksi.
Tässä lähestymistavassa on ongelmia Esimerkiksi potilaat, joilla on tiloja, jotka voivat jäljitellä GERD:tä, erityisesti pohjukaissuolen tai mahahaavan (vatsa), voivat myös todella reagoida tällaiseen hoitoon. Tässä tilanteessa, jos lääkäri olettaa, että ongelma on GERD, haavataudin syy, kuten Helicobacter pylori-niminen infektio, jää huomaamatta. (H. pylori ), tai ei-steroidiset tulehduskipulääkkeet tai tulehduskipulääkkeet (esimerkiksi ibuprofeeni), voivat myös aiheuttaa haavaumia, ja näitä sairauksia hoidettaisiin eri tavalla kuin GERD:tä.
Lisäksi, kuten missä tahansa hoidossa, lumelääkevaikutus on ehkä 20 %, mikä tarkoittaa, että 20 % potilaista reagoi lumelääkkeeseen (inaktiiviseen) pillereihin tai oikeastaan mihin tahansa hoitoon. Tämä tarkoittaa, että 20 %:lla potilaista, joilla on jokin muu syy kuin GERD (tai haavaumat), oireet vähenevät GERD-hoidon jälkeen. Näin ollen näiden potilaiden hoitovasteen (terapeuttinen tutkimus) perusteella jatkavat GERD-hoitoa, vaikka heillä ei olisikaan GERD:tä. Lisäksi heidän oireidensa todellista syytä ei selvitetä.
Ylemmän maha-suolikanavan endoskopia (tunnetaan myös nimellä esophago-gastro-duodenoscopy tai EGD) on yleinen tapa diagnosoida GERD. EGD on toimenpide, jossa putki, joka sisältää optisen järjestelmän visualisointia varten, niellään. Kun putki etenee maha-suolikanavaa pitkin, ruokatorven, mahan ja pohjukaissuolen limakalvoja voidaan tutkia.
Useimpien refluksioireista kärsivien potilaiden ruokatorvi näyttää normaalilta. Siksi useimmilla potilailla endoskopia ei auta GERD:n diagnosoinnissa. Joskus ruokatorven limakalvo näyttää kuitenkin tulehtuneelta (esofagiitti). Lisäksi, jos havaitaan eroosiota (pinnallisia murtumia ruokatorven limakalvossa) tai haavaumia (syvempiä vaurioita limakalvossa), GERD-diagnoosi voidaan tehdä luotettavasti. Endoskopia tunnistaa myös useita GERD:n komplikaatioita, erityisesti haavaumat, ahtaumat ja Barrettin ruokatorven. Myös biopsiat voidaan ottaa.
Lopuksi EGD:llä voidaan diagnosoida muita yleisiä ongelmia, jotka voivat aiheuttaa GERD:n kaltaisia oireita (esim. haavaumat, tulehdukset tai maha- tai pohjukaissuolen syövät).
Endoskoopilla otettuja ruokatorven biopsioita ei pidetä kovin hyödyllisinä GERD:n diagnosoinnissa. Ne ovat kuitenkin käyttökelpoisia syöpien tai ruokatorven tulehduksen muiden syiden kuin happaman refluksin, erityisesti infektioiden, diagnosoinnissa. Lisäksi biopsiat ovat ainoa tapa diagnosoida Barrettin ruokatorven solumuutoksia. Viime aikoina on ehdotettu, että jopa GERD-potilailla, joiden ruokatorvi näyttävät normaaleilta silmälle, biopsiat osoittavat limakalvosolujen välisten tilojen levenemistä, mikä saattaa olla merkki vauriosta. On kuitenkin liian aikaista päätellä, että laajenemisen näkeminen on riittävän tarkkaa voidakseen olla varma GERD:n esiintymisestä.
Ennen endoskopian käyttöönottoa ruokatorven röntgenkuvaus (kutsutaan esophagrammiksi) oli ainoa tapa diagnosoida GERD. Potilaat nielivät bariumia (varjoaine), ja sitten otettiin röntgenkuvat bariumtäytteisestä ruokatorvesta. Esophagramin ongelma oli, että se oli epäherkkä testi GERD:n diagnosoimiseksi. Toisin sanoen se ei löytänyt merkkejä GERD:stä monilta potilailta, joilla oli GERD, koska potilailla oli vähän tai ei ollenkaan vaurioita ruokatorven limakalvossa. Röntgenkuvat pystyivät osoittamaan vain harvinaiset GERD:n komplikaatiot, kuten haavaumat ja ahtaumat. Röntgenkuvauksista on luovuttu GERD:n diagnosointikeinona, vaikka niistä voi edelleen olla hyötyä endoskopian ohella komplikaatioiden arvioinnissa.
Kun GERD vaikuttaa kurkkuun tai kurkunpäähän ja aiheuttaa yskän, käheyden tai kurkkukipun oireita, potilaat käyvät usein korva-, nenä- ja kurkkutautien erikoislääkärin vastaanotolla. Kurkunpään erikoislääkäri löytää usein merkkejä kurkun tai kurkunpään tulehduksesta. Vaikka kurkun tai kurkunpään sairaudet ovat yleensä tulehduksen syy, joskus GERD voi olla syynä. Näin ollen ENT-asiantuntijat yrittävät usein happoa vähentävää hoitoa vahvistaakseen GERD:n diagnoosin. Tällä lähestymistavalla on kuitenkin samat ongelmat kuin edellä on käsitelty, jotka johtuvat hoitovasteen käyttämisestä GERD:n vahvistamiseen.
Ruokatorven happotestausta pidetään "kultastandardina" GERD:n diagnosoinnissa. Kuten aiemmin on keskusteltu, hapon refluksointi on yleistä väestössä. Potilailla, joilla on GERD:n oireita tai komplikaatioita, on kuitenkin enemmän hapon refluksi kuin henkilöillä, joilla ei ole GERD:n oireita tai komplikaatioita. Lisäksi normaalit yksilöt ja GERD-potilaat voidaan erottaa kohtalaisen hyvin toisistaan sen ajan perusteella, jonka ruokatorvi sisältää happoa.
Aika, jonka ruokatorvi sisältää happoa, määritetään testillä, jota kutsutaan 24 tunnin ruokatorven pH-testiksi. (pH on matemaattinen tapa ilmaista happamuuden määrää.) Tätä testiä varten pieni putki (katetri) viedään nenän läpi ja asetetaan ruokatorveen. Katetrin kärjessä on anturi, joka tunnistaa hapon. Katetrin toinen pää tulee ulos nenästä, kietoutuu takaisin korvan yli ja kulkee alas vyötärölle, jossa se kiinnitetään tallentimeen. Joka kerta kun happo palautuu takaisin ruokatorveen mahasta, se stimuloi anturia ja tallennin tallentaa refluksijakson. Katetri poistetaan 20–24 tunnin kuluttua ja tallentimen palautusvirtausarvo analysoidaan.
pH-testin käyttämisessä GERD:n diagnosoinnissa on ongelmia. Huolimatta siitä, että normaalit yksilöt ja GERD-potilaat voidaan erottaa pH-tutkimusten perusteella melko hyvin, erottelu ei ole täydellinen. Siksi joillakin potilailla, joilla on GERD, on normaali määrä happorefluksia ja joillakin potilailla, joilla ei ole GERD:tä, on epänormaali määrä happorefluksia. Se vaatii jotain muuta kuin pH-testin vahvistamaan GERD:n esiintymistä, esimerkiksi tyypillisiä oireita, hoitovastetta tai GERD:n komplikaatioita. GERD voidaan myös luotettavasti diagnosoida, kun närästyskohtaukset korreloivat happaman refluksin kanssa, kuten happotesti osoittaa.
pH-testauksella on muutakin käyttöä GERD:n hoidossa kuin vain GERD:n diagnosoinnissa. Testi voi esimerkiksi auttaa määrittämään, miksi GERD-oireet eivät reagoi hoitoon. Ehkä 10–20 prosentilla potilaista oireet eivät parane merkittävästi GERD:n hoidossa. Tämä hoitovasteen puute voi johtua tehottomasta hoidosta. Tämä tarkoittaa, että lääke ei estä riittävästi mahan hapon tuotantoa eikä vähennä hapon refluksia. Vaihtoehtoisesti vasteen puute voidaan selittää GERD:n väärällä diagnoosilla. Molemmissa näissä tilanteissa pH-testi voi olla erittäin hyödyllinen. Jos testaus paljastaa huomattavan hapon refluksoinnin lääkityksen jatkamisen aikana, hoito on tehoton ja sitä on muutettava. Jos testaus paljastaa hyvän hapon suppression minimaalisella hapon refluksilla, GERD-diagnoosi on todennäköisesti väärä ja oireille on etsittävä muita syitä.
pH-testiä voidaan myös käyttää arvioimaan, onko refluksi oireiden (yleensä närästyksen) syy. Tämän arvioinnin tekemiseksi 24 tunnin ph-testauksen aikana potilaat kirjaavat jokaisen oireensa. Sitten, kun testiä analysoidaan, voidaan määrittää, esiintyikö happorefluksia oireiden ilmaantuessa vai ei. Jos refluksi esiintyi samaan aikaan oireiden kanssa, refluksi on todennäköisesti oireiden syy. Jos oireiden ilmaantuessa ei ollut refluksia, refluksi ei todennäköisesti ole oireiden syy.
Lopuksi pH-testiä voidaan käyttää potilaiden arvioimiseen ennen GERD:n endoskopista tai kirurgista hoitoa. Kuten edellä mainittiin, noin 20 %:lla potilaista oireet vähenevät, vaikka heillä ei ole GERD:tä (plasebovaikutus). Ennen endoskooppista tai kirurgista hoitoa on tärkeää tunnistaa nämä potilaat, koska he eivät todennäköisesti hyödy hoidoista. pH-tutkimusta voidaan käyttää näiden potilaiden tunnistamiseen, koska heillä on normaali määrä happorefluksia.
A newer method for prolonged measurement (48 hours) of acid exposure in the esophagus utilizes a small, wireless capsule that is attached to the esophagus just above the LES. The capsule is passed to the lower esophagus by a tube inserted through either the mouth or the nose. After the capsule is attached to the esophagus, the tube is removed. The capsule measures the acid refluxing into the esophagus and transmits this information to a receiver that is worn at the waist. After the study, usually after 48 hours, the information from the receiver is downloaded into a computer and analyzed. The capsule falls off of the esophagus after 3-5 days and is passed in the stool. (The capsule is not reused.)
The advantage of the capsule over standard pH testing is that there is no discomfort from a catheter that passes through the throat and nose. Moreover, with the capsule, patients look normal (they don't have a catheter protruding from their noses) and are more likely to go about their daily activities, for example, go to work, without feeling self-conscious. Because the capsule records for a longer period than the catheter (48 versus 24 hours), more data on acid reflux and symptoms are obtained. Nevertheless, it is not clear whether obtaining additional information is important.
Capsule pH testing is expensive. Sometimes the capsule does not attach to the esophagus or falls off prematurely. For periods of time the receiver may not receive signals from the capsule, and some of the information about reflux of acid may be lost. Occasionally there is pain with swallowing after the capsule has been placed, and the capsule may need to be removed endoscopically. Use of the capsule is an exciting use of new technology although it has its own specific problems.
Esophageal motility testing determines how well the muscles of the esophagus are working. For motility testing, a thin tube (catheter) is passed through a nostril, down the back of the throat, and into the esophagus. On the part of the catheter that is inside the esophagus are sensors that sense pressure. A pressure is generated within the esophagus that is detected by the sensors on the catheter when the muscle of the esophagus contracts. The end of the catheter that protrudes from the nostril is attached to a recorder that records the pressure. During the test, the pressure at rest and the relaxation of the lower esophageal sphincter are evaluated. The patient then swallows sips of water to evaluate the contractions of the esophagus.
Esophageal motility testing has two important uses in evaluating GERD. The first is in evaluating symptoms that do not respond to treatment for GERD since the abnormal function of the esophageal muscle sometimes causes symptoms that resemble the symptoms of GERD. Motility testing can identify some of these abnormalities and lead to a diagnosis of an esophageal motility disorder. The second use is evaluation prior to surgical or endoscopic treatment for GERD. In this situation, the purpose is to identify patients who also have motility disorders of the esophageal muscle. The reason for this is that in patients with motility disorders, some surgeons will modify the type of surgery they perform for GERD.
Gastric emptying studies are studies that determine how well food empties from the stomach. As discussed above, about 20 % of patients with GERD have slow emptying of the stomach that may be contributing to the reflux of acid. For gastric emptying studies, the patient eats a meal that is labeled with a radioactive substance. A sensor that is similar to a Geiger counter is placed over the stomach to measure how quickly the radioactive substance in the meal empties from the stomach.
Information from the emptying study can be useful for managing patients with GERD. For example, if a patient with GERD continues to have symptoms despite treatment with the usual medications, doctors might prescribe other medications that speed-up emptying of the stomach. Alternatively, in conjunction with GERD surgery, they might do a surgical procedure that promotes a more rapid emptying of the stomach. Nevertheless, it is still debated whether a finding of reduced gastric emptying should prompt changes in the surgical treatment of GERD.
Symptoms of nausea, vomiting, and regurgitation may be due either to abnormal gastric emptying or GERD. An evaluation of gastric emptying, therefore, may be useful in identifying patients whose symptoms are due to abnormal emptying of the stomach rather than to GERD.
The acid perfusion (Bernstein) test is used to determine if chest pain is caused by acid reflux. For the acid perfusion test, a thin tube is passed through one nostril, down the back of the throat, and into the middle of the esophagus. A dilute, acid solution and a physiologic salt solution (similar to the fluid that bathes the body's cells) are alternately poured (perfused) through the catheter and into the esophagus. The patient is unaware of which solution is being infused. If the perfusion with acid provokes the patient's usual pain and perfusion of the salt solution produces no pain, it is likely that the patient's pain is caused by acid reflux.
The acid perfusion test, however, is used only rarely. A better test for correlating pain and acid reflux is a 24-hour esophageal pH or pH capsule study during which patients note when they are having pain. It then can be determined from the pH recording if there was an episode of acid reflux at the time of the pain. This is the preferable way of deciding if acid reflux is causing a patient's pain. It does not work well, however, for patients who have infrequent pain, for example every two to three days, which may be missed by a one or two day pH study. In these cases, an acid perfusion test may be reasonable.
One of the simplest treatments for GERD is referred to as life-style changes, a combination of several changes in habit, particularly related to eating.
As discussed above, reflux of acid is more injurious at night than during the day. At night, when individuals are lying down, it is easier for reflux to occur. The reason that it is easier is because gravity is not opposing the reflux, as it does in the upright position during the day. In addition, the lack of an effect of gravity allows the refluxed liquid to travel further up the esophagus and remain in the esophagus longer. These problems can be overcome partially by elevating the upper body in bed. The elevation is accomplished either by putting blocks under the bed's feet at the head of the bed or, more conveniently, by sleeping with the upper body on a foam rubber wedge. These maneuvers raise the esophagus above the stomach and partially restore the effects of gravity. It is important that the upper body and not just the head be elevated. Elevating only the head does not raise the esophagus and fails to restore the effects of gravity.
Elevation of the upper body at night generally is recommended for all patients with GERD. Nevertheless, most patients with GERD have reflux only during the day and elevation at night is of little benefit for them. It is not possible to know for certain which patients will benefit from elevation at night unless acid testing clearly demonstrates night reflux. However, patients who have heartburn, regurgitation, or other symptoms of GERD at night are probably experiencing reflux at night and definitely should elevate their upper body when sleeping. Reflux also occurs less frequently when patients lie on their left rather than their right sides.
Several changes in eating habits can be beneficial in treating GERD. Reflux is worse following meals. This probably is so because the stomach is distended with food at that time and transient relaxations of the lower esophageal sphincter are more frequent. Therefore, smaller and earlier evening meals may reduce the amount of reflux for two reasons. First, the smaller meal results in lesser distention of the stomach. Second, by bedtime, a smaller and earlier meal is more likely to have emptied from the stomach than is a larger one. As a result, reflux is less likely to occur when patients with GERD lie down to sleep.
Certain foods are known to reduce the pressure in the lower esophageal sphincter and thereby promote reflux. These foods should be avoided and include:
Fatty foods (which should be decreased) and smoking (which should be stopped) also reduce the pressure in the sphincter and promote reflux.
In addition, patients with GERD may find that other foods aggravate their symptoms. Examples are spicy or acid-containing foods, like citrus juices, carbonated beverages, and tomato juice. These foods should also be avoided if they provoke symptoms.
One novel approach to the treatment of GERD is chewing gum. Chewing gum stimulates the production of more bicarbonate-containing saliva and increases the rate of swallowing. After the saliva is swallowed, it neutralizes acid in the esophagus. In effect, chewing gum exaggerates one of the normal processes that neutralize acid in the esophagus. It is not clear, however, how effective chewing gum is in treating heartburn. Nevertheless, chewing gum after meals is certainly worth a try.
There is a variety of over-the-counter (for example, antacids and foam barriers) and prescription medications (for example, proton pump inhibitors, histamine antagonists, and promotility drugs) for treating GERD.
Despite the development of potent medications for the treatment of GERD, antacids remain a mainstay of treatment. Antacids neutralize the acid in the stomach so that there is no acid to reflux. The problem with antacids is that their action is brief. They are emptied from the empty stomach quickly, in less than an hour, and the acid then re-accumulates. The best way to take antacids, therefore, is approximately one hour after meals, which is just before the symptoms of reflux begin after a meal. Since the food from meals slows the emptying from the stomach, an antacid taken after a meal stays in the stomach longer and is effective longer. For the same reason, a second dose of antacids approximately two hours after a meal takes advantage of the continuing post-meal slower emptying of the stomach and replenishes the acid-neutralizing capacity within the stomach.
Antacids may be aluminum, magnesium, or calcium-based. Calcium-based antacids (usually calcium carbonate), unlike other antacids, stimulate the release of gastrin from the stomach and duodenum. Gastrin is the hormone that is primarily responsible for the stimulation of acid secretion by the stomach. Therefore, the secretion of acid rebounds after the direct acid-neutralizing effect of the calcium carbonate is exhausted. The rebound is due to the release of gastrin, which results in an overproduction of acid. Theoretically at least, this increased acid is not good for GERD.
Acid rebound, however, is not clinically important. That is, treatment with calcium carbonate is not less effective or safe than treatment with antacids not containing calcium carbonate. Nevertheless, the phenomenon of acid rebound is theoretically harmful. In practice, therefore, calcium-containing antacids such as Tums and Rolaids are not recommended for frequent use. The occasional use of these calcium carbonate-containing antacids, however, is not believed to be harmful. The advantages of calcium carbonate-containing antacids are their low cost, the calcium they add to the diet, and their convenience as compared to liquids.
Aluminum-containing antacids tend to cause constipation, while magnesium-containing antacids tend to cause diarrhea. If diarrhea or constipation becomes a problem, it may be necessary to switch antacids, or use antacids containing both aluminum and magnesium.
Although antacids can neutralize acid, they do so for only a short period. For substantial neutralization of acid throughout the day, antacids would need to be given frequently, at least every hour.
The first medication developed for the more effective and convenient treatment of acid-related diseases, including GERD, was a histamine antagonist, specifically cimetidine (Tagamet). Histamine is an important chemical because it stimulates acid production by the stomach. Released within the wall of the stomach, histamine attaches to receptors (binders) on the stomach's acid-producing cells and stimulates the cells to produce acid. Histamine antagonists work by blocking the receptor for histamine and thereby preventing histamine from stimulating the acid-producing cells. (Histamine antagonists are referred to as H2 antagonists because the specific receptor they block is the histamine type 2 receptor.)
As histamine is particularly important for the stimulation of acid after meals, H2 antagonists are best taken 30 minutes before meals. The reason for this timing is so that the H2 antagonists will be at peak levels in the body after the meal when the stomach is actively producing acid. H2 antagonists also can be taken at bedtime to suppress the nighttime production of acid.
H2 antagonists are very good for relieving the symptoms of GERD, particularly heartburn. However, they are not very good for healing the inflammation (esophagitis) that may accompany GERD. They are used primarily for the treatment of heartburn in GERD that is not associated with inflammation or complications, such as erosions or ulcers, strictures, or Barrett's esophagus.
Three different H2 antagonists are available by prescription, including cimetidine (Tagamet), nizatidine (Axid), and famotidine (Pepcid). Two of these, cimetidine (Tagamet HB) and famotidine (Pepcid AC, Zantac 360) are available over-the-counter (OTC), without the need for a prescription. However, the OTC dosages are lower than those available by prescription.
The second type of drug developed specifically for acid-related diseases, such as GERD, was a proton pump inhibitor (PPI), specifically, omeprazole (Prilosec). A PPI blocks the secretion of acid into the stomach by the acid-secreting cells. The advantage of a PPI over an H2 antagonist is that the PPI shuts off acid production more completely and for a longer period of time. Not only is the PPI good for treating the symptom of heartburn, but it also is good for protecting the esophagus from acid so that esophageal inflammation can heal.
PPIs are used when H2 antagonists do not relieve symptoms adequately or when complications of GERD such as erosions or ulcers, strictures, or Barrett's esophagus exist. Five different PPIs are approved for the treatment of GERD, including omeprazole (Prilosec, Dexilant), lansoprazole (Prevacid), rabeprazole (Aciphex), pantoprazole (Protonix), and esomeprazole (Nexium), and dexlansoprazole (Dexilant). A sixth PPI product consists of a combination of omeprazole and sodium bicarbonate (Zegerid). PPIs (except for Zegerid) are best taken an hour before meals. The reason for this timing is that the PPIs work best when the stomach is most actively producing acid, which occurs after meals. If the PPI is taken before the meal, it is at peak levels in the body after the meal when the acid is being made.
Pro-motility drugs work by stimulating the muscles of the gastrointestinal tract, including the esophagus, stomach, small intestine, and/or colon. One pro-motility drug, metoclopramide (Reglan), is approved for GERD. Pro-motility drugs increase the pressure in the lower esophageal sphincter and strengthen the contractions (peristalsis) of the esophagus. Both effects would be expected to reduce the reflux of acid. However, these effects on the sphincter and esophagus are small. Therefore, it is believed that the primary effect of metoclopramide may be to speed up emptying of the stomach, which also would be expected to reduce reflux.
Pro-motility drugs are most effective when taken 30 minutes before meals and again at bedtime. They are not very effective for treating either the symptoms or complications of GERD. Therefore, the pro-motility agents are reserved either for patients who do not respond to other treatments or are added to enhance other treatments for GERD.
Foam barriers provide a unique form of treatment for GERD. Foam barriers are tablets that are composed of an antacid and a foaming agent. As the tablet disintegrates and reaches the stomach, it turns into foam that floats on top of the liquid contents of the stomach. The foam forms a physical barrier to the reflux of liquid. At the same time, the antacid bound to the foam neutralizes acid that comes into contact with the foam. The tablets are best taken after meals (when the stomach is distended) and when lying down, both times when reflux is more likely to occur. Foam barriers are not often used as the first or only treatment for GERD. Rather, they are added to other drugs for GERD when the other drugs are not adequately effective in relieving symptoms. There is only one foam barrier, which is a combination of aluminum hydroxide gel, magnesium trisilicate, and alginate (Gaviscon).
The drugs described above usually are effective in treating the symptoms and complications of GERD. Nevertheless, sometimes they are not. For example, despite adequate suppression of acid and relief from heartburn, regurgitation, with its potential for complications in the lungs, may still occur. Moreover, the amounts and/or numbers of drugs that are required for satisfactory treatment are sometimes so great that drug treatment is unreasonable. In such situations, surgery can effectively stop reflux.
The surgical procedure that is done to prevent reflux is technically known as fundoplication and is called reflux surgery or anti-reflux surgery. During fundoplication, any hiatal hernial sac is pulled below the diaphragm and stitched there. In addition, the opening in the diaphragm through which the esophagus passes is tightened around the esophagus. Finally, the upper part of the stomach next to the opening of the esophagus into the stomach is wrapped around the lower esophagus to make an artificial lower esophageal sphincter. All of this surgery can be done through an incision in the abdomen (laparotomy) or using a technique called laparoscopy. During laparoscopy, a small viewing device and surgical instruments are passed through several small puncture sites in the abdomen. This procedure avoids the need for a major abdominal incision.
Surgery is very effective at relieving symptoms and treating the complications of GERD. Approximately 80% of patients will have good or excellent relief of their symptoms for at least 5 to 10 years. Nevertheless, many patients who have had surgery will continue to take drugs for reflux. It is not clear whether they take the drugs because they continue to have reflux and symptoms of reflux or if they take them for symptoms that are being caused by problems other than GERD. The most common complication of fundoplication is swallowed food that sticks at the artificial sphincter. Fortunately, the sticking usually is temporary. If it is not transient, endoscopic treatment to stretch (dilate) the artificial sphincter usually will relieve the problem. Only occasionally is it necessary to re-operate to revise the prior surgery.
Very recently, endoscopic techniques for the treatment of GERD have been developed and tested. One type of endoscopic treatment involves suturing (stitching) the area of the lower esophageal sphincter, which essentially tightens the sphincter.
A second type involves the application of radio-frequency waves to the lower part of the esophagus just above the sphincter. The waves cause damage to the tissue beneath the esophageal lining and a scar (fibrosis) forms. The scar shrinks and pulls on the surrounding tissue, thereby tightening the sphincter and the area above it.
A third type of endoscopic treatment involves the injection of materials into the esophageal wall in the area of the LES. The injected material is intended to increase pressure in the LES and thereby prevent reflux. In one treatment the injected material was a polymer. Unfortunately, the injection of polymer led to serious complications, and the material for injection is no longer available. Another treatment involving injection of expandable pellets also was discontinued. Limited information is available about a third type of injection which uses gelatinous polymethylmethacrylate microspheres.
Endoscopic treatment has the advantage of not requiring surgery. It can be performed without hospitalization. Experience with endoscopic techniques is limited. It is not clear how effective they are, especially long-term. Because the effectiveness and the full extent of potential complications of endoscopic techniques are not clear, it is felt generally that endoscopic treatment should only be done as part of experimental trials.
Transient LES relaxations appear to be the most common way in which acid reflux occurs. Although there is an available drug that prevents relaxations (baclofen), it has side effects that are too frequent to be generally useful. Much attention is being directed at the development of drugs that prevent these relaxations without accompanying side effects.
There are several ways to approach the evaluation and management of GERD. The approach depends primarily on the frequency and severity of symptoms, the adequacy of the response to treatment, and the presence of complications.
For infrequent heartburn, the most common symptom of GERD, life-style changes and an occasional antacid may be all that is necessary. If heartburn is frequent, daily non-prescription-strength (over-the-counter) H2 antagonists may be adequate. A foam barrier also can be used with the antacid or H2 antagonist.
If life-style changes and antacids, non-prescription H2 antagonists, and a foam barrier do not adequately relieve heartburn, it is time to see a physician for further evaluation and to consider prescription-strength drugs. The evaluation by the physician should include an assessment for possible complications of GERD based on the presence of such symptoms or findings as:
Clues to the presence of diseases that may mimic GERD, such as gastric or duodenal ulcers and esophageal motility disorders, should be sought.
If there are no symptoms or signs of complications and no suspicion of other diseases, a therapeutic trial of acid suppression with H2 antagonists often is used. If H2 antagonists are not adequately effective, a second trial, with the more potent PPIs, can be given. Sometimes, a trial of treatment begins with a PPI and skips the H2 antagonist. If treatment relieves the symptoms completely, no further evaluation may be necessary and the effective drug, the H2 antagonist or PPI, is continued. As discussed previously, however, there are potential problems with this commonly used approach, and some physicians would recommend a further evaluation for almost all patients they see.
If at the time of evaluation, there are symptoms or signs that suggest complicated GERD or a disease other than GERD or if the relief of symptoms with H2 antagonists or PPIs is not satisfactory, a further evaluation by endoscopy (EGD) definitely should be done.
There are several possible results of endoscopy and each requires a different approach to treatment. If the esophagus is normal and no other diseases are found, the goal of treatment simply is to relieve symptoms. Therefore, prescription strength H2 antagonists or PPIs are appropriate. If damage to the esophagus (esophagitis or ulceration) is found, the goal of treatment is healing the damage. In this case, PPIs are preferred over H2 antagonists because they are more effective for healing.
If complications of GERD, such as stricture or Barrett's esophagus are found, treatment with PPIs also is more appropriate. However, the adequacy of the PPI treatment probably should be evaluated with a 24-hour pH study during treatment with the PPI. (With PPIs, although the amount of acid reflux may be reduced enough to control symptoms, it may still be abnormally high. Therefore, judging the adequacy of suppression of acid reflux by only the response of symptoms to treatment is not satisfactory.) Strictures may also need to be treated by endoscopic dilatation (widening) of the esophageal narrowing. With Barrett's esophagus, periodic endoscopic examination should be done to identify pre-malignant changes in the esophagus.
If symptoms of GERD do not respond to maximum doses of PPI, there are two options for management. The first is to perform 24-hour pH testing to determine whether the PPI is ineffective or if a disease other than GERD is likely to be present. If the PPI is ineffective, a higher dose of PPI may be tried. The second option is to go ahead without 24 hour pH testing and to increase the dose of PPI. Another alternative is to add another drug to the PPI that works in a way that is different from the PPI, for example, a pro-motility drug or a foam barrier. If necessary, all three types of drugs can be used. If there is not a satisfactory response to this maximal treatment, 24 hour pH testing should be done.
Who should consider surgery or, perhaps, an endoscopic treatment trial for GERD? (As mentioned previously, the effectiveness of the recently developed endoscopic treatments remains to be determined.) Patients should consider surgery if they have regurgitation that cannot be controlled with drugs. This recommendation is particularly important if the regurgitation results in infections in the lungs or occurs at night when aspiration into the lungs is more likely. Patients also should consider surgery if they require large doses of PPI or multiple drugs to control their reflux. It is debated whether or not a desire to be free of the need to take life-long drugs to prevent symptoms of GERD is by itself a satisfactory reason for having surgery.
Some physicians - primarily surgeons - recommend that all patients with Barrett's esophagus should have surgery. This recommendation is based on the belief that surgery is more effective than endoscopic surveillance or ablation of the abnormal tissue followed by treatment with acid-suppressing drugs in preventing both the reflux and the cancerous changes in the esophagus. There are no studies, however, demonstrating the superiority of surgery over drugs or ablation for the treatment of GERD and its complications. Moreover, the effectiveness of drug treatment can be monitored with 24 hour pH testing.
One unresolved issue in GERD is the inconsistent relationships among acid reflux, heartburn, and damage to the lining of the esophagus (esophagitis and the complications).
Clearly, we have much to learn about the relationship between acid reflux and esophageal damage, and about the processes (mechanisms) responsible for heartburn. This issue is of more than passing interest. Knowledge of the mechanisms that produce heartburn and esophageal damage raises the possibility of new treatments that would target processes other than acid reflux.
One of the more interesting theories that has been proposed to answer some of these questions involves the reason for pain when acid refluxes. It often is assumed that the pain is caused by irritating acid contacting an inflamed esophageal lining. But the esophageal lining usually is not inflamed. It is possible therefore, that the acid is stimulating the pain nerves within the esophageal wall just beneath the lining. Although this may be the case, a second explanation is supported by the work of one group of scientists. These scientists find that heartburn provoked by acid in the esophagus is associated with contraction of the muscle in the lower esophagus. Perhaps it is the contraction of the muscle that somehow leads to the pain. It also is possible, however, that the contraction is an epiphenomenon, that is, refluxed acid stimulates pain nerves and causes the muscle to contract, but it is not the contraction that causes the pain. More studies will be necessary before the exact mechanism(s) that causes heartburn is clear.
There are potentially injurious agents that can be refluxed other than acid, for example, bile. Until recently it has been impossible or difficult to accurately identify non-acid reflux and, therefore, to study whether or not non-acid reflux is injurious or can cause symptoms.
A new technology allows the accurate determination of non-acid reflux. This technology uses the measurement of impedance changes within the esophagus to identify reflux of liquid, be it acid or non-acid. By combining measurement of impedance and pH it is possible to identify reflux and to tell if the reflux is acid or non-acid. It is too early to know how important non-acid reflux is in causing esophageal damage, symptoms, or complications, but there is little doubt that this new technology will be able to resolve the issues surrounding non-acid reflux.
 Suuhygienia ja COVID-19:n vakavuus-yhteys
Brittiläiset tutkijat ovat löytäneet yhteyden huonon suuhygienian ja vakavan akuutin hengitystieoireyhtymän koronavirus 2 (SARS-CoV-2) -infektion aiheuttaman COVID-19-taudin vakavuuden välillä. Tutkij
Suuhygienia ja COVID-19:n vakavuus-yhteys
Brittiläiset tutkijat ovat löytäneet yhteyden huonon suuhygienian ja vakavan akuutin hengitystieoireyhtymän koronavirus 2 (SARS-CoV-2) -infektion aiheuttaman COVID-19-taudin vakavuuden välillä. Tutkij
 Haluatko auttaa ihmisiä ja saada palkkaa?
Ilman voittoa menetimme 14 876 dollaria ja itkin. Vihasin päivätyötäni ja SCD Lifestyle menetti edelleen rahaa. Olin kyllästynyt 80-100 tunnin työskentelyyn viikossa. Ja Jordan ja minä romutimme oh
Haluatko auttaa ihmisiä ja saada palkkaa?
Ilman voittoa menetimme 14 876 dollaria ja itkin. Vihasin päivätyötäni ja SCD Lifestyle menetti edelleen rahaa. Olin kyllästynyt 80-100 tunnin työskentelyyn viikossa. Ja Jordan ja minä romutimme oh
 9 ummetuksen syytä ja pitkäaikaisen ummetuksen lähteitä
Kun sinulla on pitkäaikainen ummetus, suolistosi kertoo, että jotain on muutettava. Löydä yhdeksän yleistä ummetuksen syytä ja milloin kysyä lääkäriltä. Sisällysluettelo 1. Kuivuminen ja ummetus 2.
9 ummetuksen syytä ja pitkäaikaisen ummetuksen lähteitä
Kun sinulla on pitkäaikainen ummetus, suolistosi kertoo, että jotain on muutettava. Löydä yhdeksän yleistä ummetuksen syytä ja milloin kysyä lääkäriltä. Sisällysluettelo 1. Kuivuminen ja ummetus 2.





