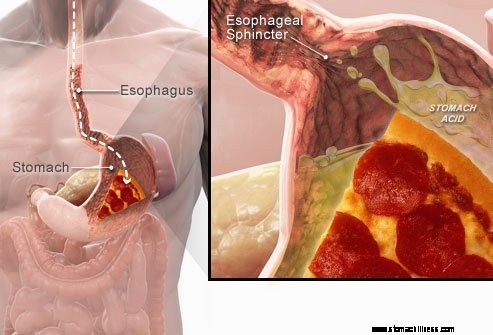
 Keď prehĺtate jedlo, putuje dolu pažerákom a prechádza cez svalový prstenec známy ako dolný pažerákový zvierač ( LES). Táto štruktúra sa otvára, aby umožnila potrave prejsť do žalúdka. Predpokladá sa, že zostane uzavretá, aby obsah žalúdka zostal tam, kam patrí.
Keď prehĺtate jedlo, putuje dolu pažerákom a prechádza cez svalový prstenec známy ako dolný pažerákový zvierač ( LES). Táto štruktúra sa otvára, aby umožnila potrave prejsť do žalúdka. Predpokladá sa, že zostane uzavretá, aby obsah žalúdka zostal tam, kam patrí.
GERD alebo symptómy refluxu kyseliny sú spôsobené regurgitáciou kyslého tekutého žalúdočného obsahu späť do pažeráka. Najčastejším príznakom GERD je pálenie záhy.
Ďalšie príznaky, ktoré sa môžu vyskytnúť v dôsledku GERD, zahŕňajú:
 Najčastejším príznakom GERD je pálenie záhy.
Najčastejším príznakom GERD je pálenie záhy. Gastroezofageálna refluxná choroba, bežne označovaná ako GERD alebo kyslý reflux, je stav, pri ktorom tekutý obsah žalúdka regurgituje (zálohuje alebo refluxuje) do pažeráka. Kvapalina môže zapáliť a poškodiť výstelku (ezofagitída), hoci viditeľné známky zápalu sa vyskytujú u menšiny pacientov. Regurgitovaná tekutina zvyčajne obsahuje kyselinu a pepsín, ktoré produkuje žalúdok. (Pepsín je enzým, ktorý začína trávenie bielkovín v žalúdku.) Refluxovaná tekutina môže obsahovať aj žlč, ktorá sa do žalúdka vrátila z dvanástnika. Prvá časť tenkého čreva pripojená k žalúdku. Predpokladá sa, že kyselina je najškodlivejšou zložkou refluxovanej kvapaliny. Pepsín a žlč môžu tiež poškodiť pažerák, ale ich úloha pri vzniku zápalu a poškodenia pažeráka nie je taká jasná ako úloha kyseliny.
GERD je chronický stav. Akonáhle to začne, je to zvyčajne na celý život. Ak dôjde k poraneniu sliznice pažeráka (ezofagitída), ide tiež o chronický stav. Navyše, po zahojení pažeráka liečbou a ukončení liečby sa zranenie u väčšiny pacientov v priebehu niekoľkých mesiacov vráti. Akonáhle sa liečba GERD začne, bude potrebné v nej pokračovať na neurčito. Niektorí pacienti s intermitentnými symptómami a bez ezofagitídy však môžu byť liečení iba počas symptomatických období.
V skutočnosti sa u väčšiny normálnych jedincov vyskytuje reflux tekutého obsahu žalúdka do pažeráka. Jedna štúdia zistila, že reflux sa často vyskytuje u normálnych jedincov ako u pacientov s GERD. U pacientov s GERD však refluxovaná tekutina obsahuje kyselinu častejšie a kyselina zostáva v pažeráku dlhšie. Zistilo sa tiež, že u pacientov s GERD dochádza k refluxu tekutín na vyššiu úroveň v pažeráku ako u normálnych jedincov.
Ako to už často býva, telo má spôsoby, ako sa chrániť pred škodlivými účinkami refluxu a kyseliny. Napríklad väčšina refluxu sa vyskytuje počas dňa, keď sú jednotlivci vzpriamení. Vo vzpriamenej polohe je pravdepodobnejšie, že refluxovaná tekutina stečie späť do žalúdka v dôsledku účinku gravitácie. Navyše, kým sú jedinci bdelí, opakovane prehĺtajú, či už je alebo nie je reflux. Každé prehltnutie nesie akúkoľvek refluxovanú tekutinu späť do žalúdka. Nakoniec slinné žľazy v ústach produkujú sliny, ktoré obsahujú hydrogénuhličitan. Pri každom prehltnutí putujú sliny obsahujúce bikarbonát do pažeráka. Hydrogénuhličitan neutralizuje malé množstvo kyseliny, ktoré zostáva v pažeráku potom, čo gravitácia a prehĺtanie odstráni väčšinu kyslej tekutiny.
Gravitácia, prehĺtanie a sliny sú dôležitými ochrannými mechanizmami pažeráka, ale sú účinné iba vtedy, keď sú jednotlivci vo vzpriamenej polohe. V noci počas spánku gravitácia nemá vplyv, prehĺtanie sa zastaví, sekrécia slín sa zníži. Preto je pravdepodobnejšie, že reflux, ktorý sa vyskytuje v noci, bude mať za následok, že kyselina zostane v pažeráku dlhšie a spôsobí väčšie poškodenie pažeráka.
Určité podmienky spôsobujú, že osoba je náchylná na GERD. Napríklad GERD môže byť vážnym problémom počas tehotenstva. Zvýšené hladiny hormónov v tehotenstve pravdepodobne spôsobujú reflux znížením tlaku v dolnom pažerákovom zvierači (pozri nižšie). Rastúci plod zároveň zvyšuje tlak v brušku. Očakáva sa, že oba tieto účinky zvýšia reflux. Tiež pacienti s ochoreniami, ktoré oslabujú svaly pažeráka, ako je sklerodermia alebo zmiešané ochorenia spojivového tkaniva, sú náchylnejší na rozvoj GERD.
Príčina GERD je komplexná a môže zahŕňať viacero príčin. Okrem toho môžu rôzne príčiny ovplyvniť rôznych jednotlivcov alebo dokonca toho istého jednotlivca v rôznych časoch. Malý počet pacientov s GERD produkuje abnormálne veľké množstvá kyseliny, ale je to nezvyčajné a neprispievajúci faktor u veľkej väčšiny pacientov.
Faktory, ktoré prispievajú k GERD, sú:
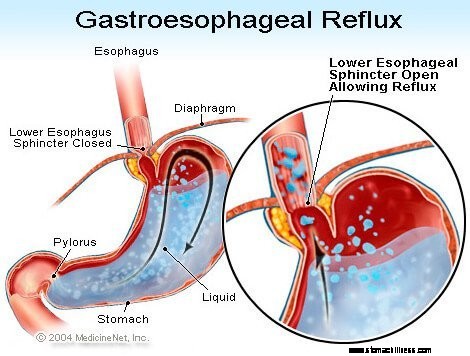
Pôsobenie dolného pažerákového zvierača (LES) je možno najdôležitejším faktorom (mechanizmom) na predchádzanie refluxu. Pažerák je svalová trubica, ktorá sa tiahne od spodnej časti hrdla až po žalúdok. LES je špecializovaný prstenec svalov, ktorý obklopuje najspodnejší koniec pažeráka, kde sa spája so žalúdkom. Sval tvoriaci LES je aktívny väčšinu času, teda v pokoji. To znamená, že sa sťahuje a uzatvára priechod z pažeráka do žalúdka. Toto uzavretie priechodu zabraňuje refluxu. Keď sa jedlo alebo sliny prehltnú, LES sa na niekoľko sekúnd uvoľní, aby jedlo alebo sliny prešli z pažeráka do žalúdka, a potom sa opäť uzavrie.
U pacientov s GERD sa zistilo niekoľko rôznych abnormalít LES. Dve z nich zahŕňajú funkciu LES. Prvým je abnormálne slabá kontrakcia LES, ktorá znižuje jeho schopnosť zabrániť refluxu. Druhým sú abnormálne relaxácie LES, nazývané prechodné relaxácie LES. Abnormálne sú v tom, že nesprevádzajú lastovičky a trvajú dlho, až niekoľko minút. Tieto predĺžené relaxácie umožňujú ľahší výskyt refluxu. Prechodné relaxácie LES sa vyskytujú u pacientov s GERD najčastejšie po jedle, keď je žalúdok roztiahnutý jedlom. Prechodné relaxácie LES sa vyskytujú aj u jedincov bez GERD, ale nie sú časté.
Najnovšie opísaná abnormalita u pacientov s GERD je laxnosť LES. Konkrétne, podobné distinkčné tlaky otvárajú LES viac u pacientov s GERD ako u jedincov bez GERD. Aspoň teoreticky by to umožnilo ľahšie otvorenie LES a/alebo väčší spätný tok kyseliny do pažeráka, keď je LES otvorený.
Hiátové prietrže prispievajú k refluxu, hoci spôsob, akým prispievajú, nie je jasný. Väčšina pacientov s GERD má hiátovú herniu, ale mnohí ju nemajú. Preto nie je potrebné mať hiátovú herniu, aby ste mali GERD. Navyše, veľa ľudí má hiátovú herniu, ale nemajú GERD. Nie je s určitosťou známe, ako alebo prečo sa hiátová prietrž vyvíja.
Normálne sa LES nachádza na rovnakej úrovni, kde pažerák prechádza z hrudníka cez malý otvor v bránici a do brucha. (Membrána je svalová horizontálna prepážka, ktorá oddeľuje hrudník od brucha.) Keď dôjde k hiátovej prietrži, malá časť hornej časti žalúdka, ktorá sa pripája k pažeráku, tlačí nahor cez bránicu. Výsledkom je, že malá časť žalúdka a LES ležia v hrudníku a LES už nie je na úrovni bránice.
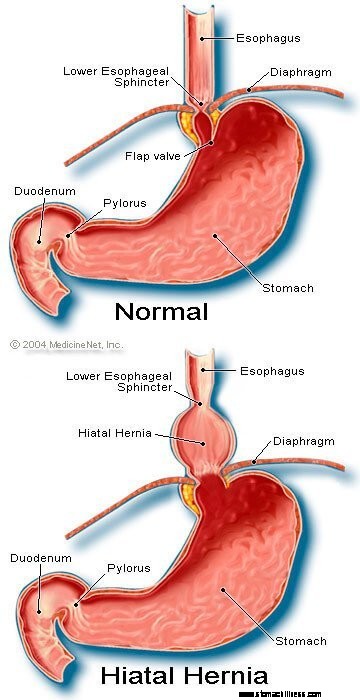 Obrázok hiátovej hernie
Obrázok hiátovej hernie
Zdá sa, že bránica, ktorá obklopuje LES, je dôležitá pri prevencii refluxu. To znamená, že u jedincov bez hiátových hernií je bránica obklopujúca pažerák nepretržite stiahnutá, ale potom sa uvoľňuje prehĺtaním, rovnako ako LES. Všimnite si, že účinky LES a bránice sa vyskytujú na rovnakom mieste u pacientov bez hiátových hernií. Preto sa bariéra refluxu rovná súčtu tlakov generovaných LES a membránou. Keď sa LES presunie do hrudníka s hiátovou prietržou, bránica a LES naďalej vyvíjajú svoj tlak a bariérový efekt. Teraz to však robia na rôznych miestach. V dôsledku toho už tlaky nie sú aditívne. Namiesto toho je jedna vysokotlaková bariéra refluxu nahradená dvomi bariérami nižšieho tlaku a reflux tak nastáva ľahšie. Takže zníženie tlakovej bariéry je jedným zo spôsobov, ako môže hiátová hernia prispieť k refluxu.
Ako už bolo spomenuté, lastovičky sú dôležité pri odstraňovaní kyseliny v pažeráku. Prehĺtanie spôsobuje prstencovú vlnu kontrakcie pažerákových svalov, ktorá zužuje lúmen (vnútornú dutinu) pažeráka. Sťah, označovaný ako peristaltika, začína v hornom pažeráku a postupuje do dolného pažeráka. Tlačí jedlo, sliny a čokoľvek iné v pažeráku do žalúdka.
Keď je vlna kontrakcie chybná, refluxovaná kyselina sa netlačí späť do žalúdka. U pacientov s GERD bolo popísaných niekoľko abnormalít kontrakcie. Napríklad vlny kontrakcií nemusia začať po každom prehltnutí alebo vlny kontrakcií môžu odznieť skôr, ako sa dostanú do žalúdka. Tiež tlak vytvorený kontrakciami môže byť príliš slabý na to, aby vytlačil kyselinu späť do žalúdka. Takéto abnormality kontrakcie, ktoré znižujú klírens kyseliny z pažeráka, sa často vyskytujú u pacientov s GERD. V skutočnosti sa najčastejšie vyskytujú u pacientov s najzávažnejším GERD. Očakávalo by sa, že účinky abnormálnych kontrakcií pažeráka budú horšie v noci, keď gravitácia nepomáha vrátiť refluxovanú kyselinu do žalúdka. Všimnite si, že fajčenie tiež podstatne znižuje klírens kyseliny z pažeráka. Tento účinok pretrváva najmenej 6 hodín po poslednej cigarete.
Väčšina refluxu počas dňa sa vyskytuje po jedle. Tento reflux je pravdepodobne spôsobený prechodnými relaxáciami LES, ktoré sú spôsobené roztiahnutím žalúdka s jedlom. Zistilo sa, že približne u menšiny pacientov s GERD sa žalúdky po jedle vyprázdňujú abnormálne pomaly. Toto sa nazýva gastroparéza. Pomalšie vyprázdňovanie žalúdka predlžuje roztiahnutie žalúdka s jedlom po jedle. Preto pomalšie vyprázdňovanie predlžuje dobu, počas ktorej je pravdepodobnejší výskyt refluxu. Existuje niekoľko liekov spojených so zhoršeným vyprázdňovaním žalúdka, ako napríklad:
Jednotlivci by nemali prestať užívať tieto ani žiadne lieky, ktoré im boli predpísané, kým s nimi predpisujúci lekár nepreberie možnú situáciu GERD.
Príznaky nekomplikovanej GERD sú predovšetkým:
Ďalšie príznaky sa vyskytujú, keď sa vyskytnú komplikácie GERD a budú prediskutované s komplikáciami.
Keď sa u pacientov s GERD vracia kyselina späť do pažeráka, stimulujú sa nervové vlákna v pažeráku. Táto nervová stimulácia vedie najčastejšie k páleniu záhy, bolesti, ktorá je charakteristická pre GERD. Pálenie záhy sa zvyčajne popisuje ako pálivá bolesť v strede hrudníka. Môže začať vysoko v bruchu alebo sa môže rozšíriť až do krku. U niektorých pacientov však môže byť bolesť ostrá alebo podobná tlaku, nie pálenie. Takáto bolesť môže napodobňovať bolesť srdca (angína). U iných pacientov sa bolesť môže rozšíriť až do chrbta.
Keďže kyslý reflux je bežnejší po jedle, pálenie záhy je častejšie po jedle. Pálenie záhy je tiež bežnejšie, keď si jednotlivci ľahnú, pretože bez účinkov gravitácie sa reflux vyskytuje ľahšie a kyselina sa vracia do žalúdka pomalšie. Mnoho pacientov s GERD prebúdza zo spánku pálenie záhy.
Epizódy pálenia záhy sa vyskytujú pravidelne. To znamená, že epizódy sú častejšie alebo závažnejšie počas niekoľkých týždňov alebo mesiacov, a potom sa stávajú menej časté alebo závažné alebo dokonca chýbajú na niekoľko týždňov alebo mesiacov. Táto periodicita symptómov poskytuje dôvod na intermitentnú liečbu u pacientov s GERD, ktorí nemajú ezofagitídu. Pálenie záhy je však celoživotný problém a takmer vždy sa vráti.
Regurgitácia je výskyt refluxovanej tekutiny v ústach. U väčšiny pacientov s GERD sa do pažeráka zvyčajne dostanú len malé množstvá tekutiny a tekutina zostáva v dolnom pažeráku. Príležitostne u niektorých pacientov s GERD sú väčšie množstvá tekutiny, niekedy obsahujúce potravu, refluxované a dosahujú horný pažerák.
Na hornom konci pažeráka je horný pažerákový zvierač (UES). UES je kruhový prstenec svalu, ktorý je svojou činnosťou veľmi podobný LES. To znamená, že UES zabraňuje tomu, aby sa obsah pažeráka vrátil späť do hrdla. Keď malé množstvo refluxovanej tekutiny a/alebo jedla prenikne cez UES a dostane sa do hrdla, v ústach môže byť kyslá chuť. Ak väčšie množstvá porušia UES, pacienti môžu náhle nájsť ústa naplnené tekutinou alebo jedlom. A čo viac, častá alebo dlhotrvajúca regurgitácia môže viesť k erózii zubov vyvolanej kyselinou.
Nevoľnosť je pri GERD nezvyčajná. U niektorých pacientov však môže byť časté alebo závažné a môže viesť k zvracaniu. V skutočnosti u pacientov s nevysvetliteľnou nevoľnosťou a/alebo vracaním je GERD jednou z prvých podmienok, ktoré treba zvážiť. Nie je jasné, prečo sa u niektorých pacientov s GERD rozvinie hlavne pálenie záhy a u iných hlavne nevoľnosť.
Kvapalina zo žalúdka, ktorá sa refluxuje do pažeráka, poškodzuje bunky lemujúce pažerák. Telo reaguje tak, ako zvyčajne reaguje na poškodenie, čo je zápal (ezofagitída). Účelom zápalu je neutralizovať poškodzujúce činidlo a začať proces hojenia. Ak sa poškodenie dostane hlboko do pažeráka, vytvorí sa vred. Vred je jednoducho prerušenie sliznice pažeráka, ktoré sa vyskytuje v oblasti zápalu. Vredy a ďalší zápal, ktorý vyvolávajú, môžu erodovať do krvných ciev pažeráka a spôsobiť krvácanie do pažeráka.
Príležitostne je krvácanie závažné a môže vyžadovať:
Vredy pažeráka sa hoja s tvorbou jaziev (fibróza). V priebehu času sa zjazvené tkanivo zmenšuje a zužuje lúmen (vnútorná dutina) pažeráka. Toto zjazvené zúženie sa nazýva striktúra. Prehltnuté jedlo môže uviaznuť v pažeráku, keď sa zúženie stane dostatočne závažným (zvyčajne, keď obmedzí lúmen pažeráka na priemer jeden centimeter). Táto situácia si môže vyžiadať endoskopické odstránenie zaseknutého jedla. Potom, aby sa jedlo nelepilo, treba zúženie natiahnuť (rozšíriť). Okrem toho, aby sa predišlo recidíve striktúry, musí sa zabrániť aj refluxu.
Dlhodobá a/alebo závažná GERD spôsobuje u niektorých pacientov zmeny v bunkách, ktoré lemujú pažerák. Tieto bunky sú predrakovinové a môžu sa, hoci zvyčajne, stať rakovinovými. Tento stav sa označuje ako Barrettov pažerák a vyskytuje sa približne u 10 % pacientov s GERD. Typ rakoviny pažeráka spojený s Barrettovým pažerákom (adenokarcinóm) sa zvyšuje. Nie je jasné, prečo sa u niektorých pacientov s GERD rozvinie Barrettov pažerák, ale u väčšiny nie.
Barrettov pažerák možno rozpoznať vizuálne v čase endoskopie a potvrdiť mikroskopickým vyšetrením buniek výstelky. Potom môžu pacienti s Barrettovým pažerákom pravidelne podstupovať endoskopické kontroly s biopsiami, hoci neexistuje zhoda v tom, ktorí pacienti vyžadujú sledovanie. Účelom sledovania je odhaliť progresiu od predrakovinových k viac rakovinovým zmenám, aby bolo možné začať s liečbou prevenciou rakoviny. Tiež sa verí, že pacienti s Barrettovým pažerákom by mali dostať maximálnu liečbu GERD, aby sa zabránilo ďalšiemu poškodeniu pažeráka. Študujú sa postupy, ktoré odstraňujú abnormálne výstelkové bunky. Na odstránenie buniek možno použiť niekoľko endoskopických, nechirurgických techník. Tieto techniky sú atraktívne, pretože nevyžadujú chirurgický zákrok; sú však spojené s komplikáciami a dlhodobá účinnosť liečby ešte nebola stanovená. Chirurgické odstránenie pažeráka je vždy možnosťou.
Veľa nervov je v dolnom pažeráku. Niektoré z týchto nervov sú stimulované refluxovanou kyselinou a táto stimulácia má za následok bolesť (zvyčajne pálenie záhy). Iné nervy, ktoré sú stimulované, nevyvolávajú bolesť. Namiesto toho stimulujú ďalšie nervy, ktoré vyvolávajú kašeľ. Týmto spôsobom môže refluxovaná tekutina spôsobiť kašeľ bez toho, aby sa dostala do hrdla! Podobným spôsobom môže reflux do dolného pažeráka stimulovať pažerákové nervy, ktoré sa spájajú s a môžu stimulovať nervy smerujúce do pľúc. Tieto nervy do pľúc potom môžu spôsobiť zúženie menších dýchacích trubíc, čo vedie k záchvatu astmy.
Hoci GERD môže spôsobiť kašeľ, nie je bežnou príčinou nevysvetliteľného kašľa. Hoci GERD môže byť tiež príčinou astmy, je pravdepodobnejšie, že vyvoláva astmatické záchvaty u pacientov, ktorí už astmu majú. Hoci chronický kašeľ a astma sú bežné ochorenia, nie je jasné, ako často sa zhoršujú alebo spôsobujú GERD.
Ak sa refluxovaná tekutina dostane cez horný pažerákový zvierač, môže sa dostať do hrdla (hltanu) a dokonca aj do hlasovej schránky (hrtan). Výsledný zápal môže viesť k bolesti hrdla a chrapotu. Rovnako ako pri kašli a astme nie je jasné, ako často je GERD zodpovedný za inak nevysvetliteľný zápal hrdla a hrtana.
Refluxovaná tekutina, ktorá prechádza z hrdla (hltanu) a do hrtana, sa môže dostať do pľúc (aspirácia). Reflux tekutiny do pľúc (nazývaný aspirácia) má často za následok kašeľ a dusenie. Aspirácia však môže nastať aj bez vyvolania týchto symptómov. S týmito príznakmi alebo bez nich môže aspirácia viesť k infekcii pľúc a viesť k zápalu pľúc. Tento typ zápalu pľúc je vážny problém vyžadujúci okamžitú liečbu. Ak aspiráciu nesprevádzajú symptómy, môže to mať za následok pomalé, progresívne zjazvenie pľúc (pľúcna fibróza), ktoré možno vidieť na röntgenových snímkach hrudníka. Aspirácia je pravdepodobnejšia v noci, pretože vtedy nie sú aktívne procesy (mechanizmy), ktoré chránia pred refluxom, a reflex kašľa, ktorý chráni pľúca, tiež nie je aktívny.
Hrdlo komunikuje s nosovými priechodmi. U malých detí sa na mieste, kde sa horná časť hrdla spája s nosnými priechodmi, nachádzajú dve časti lymfatického tkaniva, nazývané adenoidy. Priechody z dutín a trubice zo stredného ucha (Eustachove trubice) ústia do zadnej časti nosných priechodov v blízkosti adenoidov. Refluxovaná kvapalina, ktorá vstupuje do horného hrdla, môže zapáliť adenoidy a spôsobiť ich opuch. Opuchnuté adenoidy potom môžu blokovať priechody z dutín a Eustachovej trubice. Keď sú dutiny a stredné uši uzavreté od nosových priechodov opuchom adenoidov, hromadí sa v nich tekutina. Toto nahromadenie tekutiny môže viesť k nepríjemným pocitom v dutinách a ušiach. Keďže adenoidy sú výrazné u malých detí a nie u dospelých, toto nahromadenie tekutiny v ušiach a prínosových dutinách sa pozoruje u detí a nie u dospelých.
Na diagnostiku a hodnotenie pacientov s GERD existuje množstvo procedúr, testov a hodnotenia symptómov (napríklad pálenie záhy).
Zvyčajným spôsobom, ako je GERD, je jeho charakteristický príznak, pálenie záhy. Pálenie záhy sa najčastejšie popisuje ako pálenie pod hrudnou kosťou (pod stredom hrudníka), ktoré sa vyskytuje po jedle a často sa zhoršuje pri ležaní. Na potvrdenie diagnózy lekári často liečia pacientov liekmi na potlačenie tvorby kyseliny v žalúdku. Ak sa potom pálenie záhy do značnej miery zmierni, diagnóza GERD sa považuje za potvrdenú. Tento prístup stanovenia diagnózy na základe odpovede symptómov na liečbu sa bežne nazýva terapeutická štúdia.
S týmto prístupom sú problémy. Napríklad pacienti, ktorí majú stavy, ktoré môžu napodobňovať GERD, konkrétne dvanástnikové alebo žalúdočné (žalúdočné) vredy, môžu tiež skutočne reagovať na takúto liečbu. V tejto situácii, ak lekár predpokladá, že problémom je GERD, príčina vredovej choroby by sa prehliadla, ako je typ infekcie nazývaný Helicobacter pylori (H. pylori ), alebo nesteroidné protizápalové lieky alebo NSAID (napríklad ibuprofén), môžu tiež spôsobiť vredy a tieto stavy by sa liečili inak ako GERD.
Okrem toho, ako pri každej liečbe, existuje možno 20 % placebo efekt, čo znamená, že 20 % pacientov bude reagovať na placebo (neaktívnu) pilulku alebo skutočne na akúkoľvek liečbu. To znamená, že u 20 % pacientov, ktorí majú príčiny svojich symptómov iné ako GERD (alebo vredy), dôjde po liečbe GERD k zníženiu symptómov. Na základe ich odpovede na liečbu (terapeutická štúdia) sa teda títo pacienti budú naďalej liečiť na GERD, aj keď nemajú GERD. Ba čo viac, skutočná príčina ich symptómov sa nebude sledovať.
Endoskopia hornej časti gastrointestinálneho traktu (tiež známa ako ezofago-gastro-duodenoskopia alebo EGD) je bežným spôsobom diagnostiky GERD. EGD je postup, pri ktorom sa prehltne trubica obsahujúca optický systém na vizualizáciu. Ako trubica postupuje nadol gastrointestinálnym traktom, je možné preskúmať výstelku pažeráka, žalúdka a dvanástnika.
Pažerák väčšiny pacientov s príznakmi refluxu vyzerá normálne. Preto u väčšiny pacientov endoskopia nepomôže pri diagnostike GERD. Niekedy sa však sliznica pažeráka javí ako zapálená (ezofagitída). Okrem toho, ak sa objavia erózie (povrchové trhliny vo výstelke pažeráka) alebo vredy (hlbšie trhliny výstelky), je možné s istotou stanoviť diagnózu GERD. Endoskopia tiež identifikuje niekoľko komplikácií GERD, konkrétne vredy, striktúry a Barrettov pažerák. Je možné získať aj biopsie.
Nakoniec, pomocou EGD možno diagnostikovať ďalšie bežné problémy, ktoré môžu spôsobovať symptómy podobné GERD (napríklad vredy, zápaly alebo rakovinu žalúdka alebo dvanástnika).
Biopsie pažeráka získané cez endoskop sa nepovažujú za veľmi užitočné na diagnostiku GERD. Sú však užitočné pri diagnostikovaní rakoviny alebo iných príčin zápalu pažeráka ako reflux kyseliny, najmä infekcií. Okrem toho sú biopsie jediným prostriedkom na diagnostikovanie bunkových zmien Barrettovho pažeráka. Nedávno sa navrhlo, že dokonca aj u pacientov s GERD, ktorých pažerák sa javí ako normálny pre oko, biopsie ukážu rozšírenie priestorov medzi bunkami výstelky, čo môže byť príznakom poškodenia. Je však príliš skoro na to, aby sme dospeli k záveru, že pozorovanie rozšírenia je dostatočne špecifické na to, aby sme si mohli byť istí, že GERD je prítomný.
Pred zavedením endoskopie bol röntgenový snímok pažeráka (nazývaný ezofagram) jediným prostriedkom na diagnostiku GERD. Pacienti prehltli bárium (kontrastný materiál) a následne sa urobili röntgenové snímky pažeráka naplneného báriom. Problém s pažerákom bol, že to bol necitlivý test na diagnostiku GERD. To znamená, že sa nepodarilo nájsť príznaky GERD u mnohých pacientov, ktorí mali GERD, pretože pacienti mali malé alebo žiadne poškodenie sliznice pažeráka. Röntgenové snímky dokázali ukázať len zriedkavé komplikácie GERD, napríklad vredy a striktúry. Röntgenové lúče boli opustené ako prostriedok diagnostiky GERD, hoci stále môžu byť užitočné spolu s endoskopiou pri hodnotení komplikácií.
Keď GERD postihuje hrdlo alebo hrtan a spôsobuje príznaky kašľa, chrapotu alebo bolesti hrdla, pacienti často navštevujú špecialistu na uši, nos a hrdlo (ENT). ORL špecialista často zistí príznaky zápalu hrdla alebo hrtana. Hoci príčinou zápalu sú zvyčajne ochorenia hrdla alebo hrtana, niekedy môže byť príčinou GERD. V súlade s tým špecialisti ORL často skúšajú liečbu potláčajúcu kyselinu, aby potvrdili diagnózu GERD. Tento prístup má však rovnaké problémy, ako sú uvedené vyššie, ktoré vyplývajú z použitia odpovede na liečbu na potvrdenie GERD.
Testovanie kyseliny pažerákovej sa považuje za „zlatý štandard“ na diagnostiku GERD. Ako bolo uvedené vyššie, reflux kyseliny je bežný v bežnej populácii. Avšak pacienti so symptómami alebo komplikáciami GERD majú reflux viac kyseliny ako jedinci bez symptómov alebo komplikácií GERD. Navyše, normálnych jedincov a pacientov s GERD možno od seba dobre odlíšiť podľa času, počas ktorého pažerák obsahuje kyselinu.
Čas, počas ktorého pažerák obsahuje kyselinu, sa určuje testom nazývaným 24-hodinový test pH pažeráka. (pH je matematický spôsob vyjadrenia množstva kyslosti.) Pri tomto teste sa malá hadička (katéter) zavedie cez nos a umiestni sa do pažeráka. Na špičke katétra je senzor, ktorý sníma kyselinu. Druhý koniec katétra vychádza z nosa, ovinie sa späť cez ucho a putuje dole k pásu, kde je pripojený k záznamníku. Zakaždým, keď sa kyselina vracia späť do pažeráka zo žalúdka, stimuluje senzor a záznamník zaznamená epizódu refluxu. Po 20 až 24 hodinách sa katéter odstráni a analyzuje sa záznam refluxu zo zapisovača.
Existujú problémy s použitím testovania pH na diagnostiku GERD. Napriek tomu, že normálnych jedincov a pacientov s GERD možno na základe pH štúdií celkom dobre oddeliť, separácia nie je dokonalá. Preto niektorí pacienti s GERD budú mať normálne množstvo kyslého refluxu a niektorí pacienti bez GERD budú mať abnormálne množstvo kyslého refluxu. Vyžaduje si niečo iné ako test pH na potvrdenie prítomnosti GERD, napríklad typické symptómy, odpoveď na liečbu alebo prítomnosť komplikácií GERD. GERD možno spoľahlivo diagnostikovať aj vtedy, keď epizódy pálenia záhy korelujú s refluxom kyseliny, ako sa ukázalo pri testovaní kyseliny.
Testovanie pH má iné využitie v manažmente GERD ako len diagnostikovanie GERD. Test môže napríklad pomôcť určiť, prečo symptómy GERD nereagujú na liečbu. Možno u 10 až 20 percent pacientov sa ich symptómy podstatne nezlepšia liečbou GERD. Tento nedostatok odpovede na liečbu môže byť spôsobený neúčinnou liečbou. To znamená, že liek dostatočne nepotláča tvorbu kyseliny v žalúdku a neznižuje reflux kyseliny. Alternatívne môže byť nedostatočná odpoveď vysvetlená nesprávnou diagnózou GERD. V oboch týchto situáciách môže byť test pH veľmi užitočný. Ak testovanie odhalí podstatný reflux kyseliny pri pokračovaní liečby, potom je liečba neúčinná a bude potrebné ju zmeniť. Ak testovanie odhalí dobrú supresiu kyseliny s minimálnym refluxom kyseliny, diagnóza GERD je pravdepodobne nesprávna a je potrebné hľadať iné príčiny symptómov.
Testovanie pH sa môže použiť aj na vyhodnotenie toho, či je reflux príčinou symptómov (zvyčajne pálenia záhy). Na vykonanie tohto hodnotenia, zatiaľ čo sa vykonáva 24-hodinové testovanie ph, pacienti zaznamenávajú zakaždým, keď majú príznaky. Potom, keď sa test analyzuje, možno určiť, či sa v čase symptómov vyskytol reflux kyseliny alebo nie. Ak sa reflux vyskytol v rovnakom čase ako symptómy, potom je reflux pravdepodobne príčinou symptómov. Ak v čase príznakov nebol žiadny reflux, potom je nepravdepodobné, že by reflux bol príčinou príznakov.
Nakoniec, testovanie pH sa môže použiť na vyhodnotenie pacientov pred endoskopickou alebo chirurgickou liečbou GERD. Ako je uvedené vyššie, približne 20 % pacientov bude mať zmiernenie symptómov, aj keď nemajú GERD (placebo efekt). Pred endoskopickou alebo chirurgickou liečbou je dôležité identifikovať týchto pacientov, pretože pravdepodobne nebudú mať prospech z liečby. Štúdia pH sa môže použiť na identifikáciu týchto pacientov, pretože budú mať normálne množstvo kyslého refluxu.
A newer method for prolonged measurement (48 hours) of acid exposure in the esophagus utilizes a small, wireless capsule that is attached to the esophagus just above the LES. The capsule is passed to the lower esophagus by a tube inserted through either the mouth or the nose. After the capsule is attached to the esophagus, the tube is removed. The capsule measures the acid refluxing into the esophagus and transmits this information to a receiver that is worn at the waist. After the study, usually after 48 hours, the information from the receiver is downloaded into a computer and analyzed. The capsule falls off of the esophagus after 3-5 days and is passed in the stool. (The capsule is not reused.)
The advantage of the capsule over standard pH testing is that there is no discomfort from a catheter that passes through the throat and nose. Moreover, with the capsule, patients look normal (they don't have a catheter protruding from their noses) and are more likely to go about their daily activities, for example, go to work, without feeling self-conscious. Because the capsule records for a longer period than the catheter (48 versus 24 hours), more data on acid reflux and symptoms are obtained. Nevertheless, it is not clear whether obtaining additional information is important.
Capsule pH testing is expensive. Sometimes the capsule does not attach to the esophagus or falls off prematurely. For periods of time the receiver may not receive signals from the capsule, and some of the information about reflux of acid may be lost. Occasionally there is pain with swallowing after the capsule has been placed, and the capsule may need to be removed endoscopically. Use of the capsule is an exciting use of new technology although it has its own specific problems.
Esophageal motility testing determines how well the muscles of the esophagus are working. For motility testing, a thin tube (catheter) is passed through a nostril, down the back of the throat, and into the esophagus. On the part of the catheter that is inside the esophagus are sensors that sense pressure. A pressure is generated within the esophagus that is detected by the sensors on the catheter when the muscle of the esophagus contracts. The end of the catheter that protrudes from the nostril is attached to a recorder that records the pressure. During the test, the pressure at rest and the relaxation of the lower esophageal sphincter are evaluated. The patient then swallows sips of water to evaluate the contractions of the esophagus.
Esophageal motility testing has two important uses in evaluating GERD. The first is in evaluating symptoms that do not respond to treatment for GERD since the abnormal function of the esophageal muscle sometimes causes symptoms that resemble the symptoms of GERD. Motility testing can identify some of these abnormalities and lead to a diagnosis of an esophageal motility disorder. The second use is evaluation prior to surgical or endoscopic treatment for GERD. In this situation, the purpose is to identify patients who also have motility disorders of the esophageal muscle. The reason for this is that in patients with motility disorders, some surgeons will modify the type of surgery they perform for GERD.
Gastric emptying studies are studies that determine how well food empties from the stomach. As discussed above, about 20 % of patients with GERD have slow emptying of the stomach that may be contributing to the reflux of acid. For gastric emptying studies, the patient eats a meal that is labeled with a radioactive substance. A sensor that is similar to a Geiger counter is placed over the stomach to measure how quickly the radioactive substance in the meal empties from the stomach.
Information from the emptying study can be useful for managing patients with GERD. For example, if a patient with GERD continues to have symptoms despite treatment with the usual medications, doctors might prescribe other medications that speed-up emptying of the stomach. Alternatively, in conjunction with GERD surgery, they might do a surgical procedure that promotes a more rapid emptying of the stomach. Nevertheless, it is still debated whether a finding of reduced gastric emptying should prompt changes in the surgical treatment of GERD.
Symptoms of nausea, vomiting, and regurgitation may be due either to abnormal gastric emptying or GERD. An evaluation of gastric emptying, therefore, may be useful in identifying patients whose symptoms are due to abnormal emptying of the stomach rather than to GERD.
The acid perfusion (Bernstein) test is used to determine if chest pain is caused by acid reflux. For the acid perfusion test, a thin tube is passed through one nostril, down the back of the throat, and into the middle of the esophagus. A dilute, acid solution and a physiologic salt solution (similar to the fluid that bathes the body's cells) are alternately poured (perfused) through the catheter and into the esophagus. The patient is unaware of which solution is being infused. If the perfusion with acid provokes the patient's usual pain and perfusion of the salt solution produces no pain, it is likely that the patient's pain is caused by acid reflux.
The acid perfusion test, however, is used only rarely. A better test for correlating pain and acid reflux is a 24-hour esophageal pH or pH capsule study during which patients note when they are having pain. It then can be determined from the pH recording if there was an episode of acid reflux at the time of the pain. This is the preferable way of deciding if acid reflux is causing a patient's pain. It does not work well, however, for patients who have infrequent pain, for example every two to three days, which may be missed by a one or two day pH study. In these cases, an acid perfusion test may be reasonable.
One of the simplest treatments for GERD is referred to as life-style changes, a combination of several changes in habit, particularly related to eating.
As discussed above, reflux of acid is more injurious at night than during the day. At night, when individuals are lying down, it is easier for reflux to occur. The reason that it is easier is because gravity is not opposing the reflux, as it does in the upright position during the day. In addition, the lack of an effect of gravity allows the refluxed liquid to travel further up the esophagus and remain in the esophagus longer. These problems can be overcome partially by elevating the upper body in bed. The elevation is accomplished either by putting blocks under the bed's feet at the head of the bed or, more conveniently, by sleeping with the upper body on a foam rubber wedge. These maneuvers raise the esophagus above the stomach and partially restore the effects of gravity. It is important that the upper body and not just the head be elevated. Elevating only the head does not raise the esophagus and fails to restore the effects of gravity.
Elevation of the upper body at night generally is recommended for all patients with GERD. Nevertheless, most patients with GERD have reflux only during the day and elevation at night is of little benefit for them. It is not possible to know for certain which patients will benefit from elevation at night unless acid testing clearly demonstrates night reflux. However, patients who have heartburn, regurgitation, or other symptoms of GERD at night are probably experiencing reflux at night and definitely should elevate their upper body when sleeping. Reflux also occurs less frequently when patients lie on their left rather than their right sides.
Several changes in eating habits can be beneficial in treating GERD. Reflux is worse following meals. This probably is so because the stomach is distended with food at that time and transient relaxations of the lower esophageal sphincter are more frequent. Therefore, smaller and earlier evening meals may reduce the amount of reflux for two reasons. First, the smaller meal results in lesser distention of the stomach. Second, by bedtime, a smaller and earlier meal is more likely to have emptied from the stomach than is a larger one. As a result, reflux is less likely to occur when patients with GERD lie down to sleep.
Certain foods are known to reduce the pressure in the lower esophageal sphincter and thereby promote reflux. These foods should be avoided and include:
Fatty foods (which should be decreased) and smoking (which should be stopped) also reduce the pressure in the sphincter and promote reflux.
In addition, patients with GERD may find that other foods aggravate their symptoms. Examples are spicy or acid-containing foods, like citrus juices, carbonated beverages, and tomato juice. These foods should also be avoided if they provoke symptoms.
One novel approach to the treatment of GERD is chewing gum. Chewing gum stimulates the production of more bicarbonate-containing saliva and increases the rate of swallowing. After the saliva is swallowed, it neutralizes acid in the esophagus. In effect, chewing gum exaggerates one of the normal processes that neutralize acid in the esophagus. It is not clear, however, how effective chewing gum is in treating heartburn. Nevertheless, chewing gum after meals is certainly worth a try.
There is a variety of over-the-counter (for example, antacids and foam barriers) and prescription medications (for example, proton pump inhibitors, histamine antagonists, and promotility drugs) for treating GERD.
Despite the development of potent medications for the treatment of GERD, antacids remain a mainstay of treatment. Antacids neutralize the acid in the stomach so that there is no acid to reflux. The problem with antacids is that their action is brief. They are emptied from the empty stomach quickly, in less than an hour, and the acid then re-accumulates. The best way to take antacids, therefore, is approximately one hour after meals, which is just before the symptoms of reflux begin after a meal. Since the food from meals slows the emptying from the stomach, an antacid taken after a meal stays in the stomach longer and is effective longer. For the same reason, a second dose of antacids approximately two hours after a meal takes advantage of the continuing post-meal slower emptying of the stomach and replenishes the acid-neutralizing capacity within the stomach.
Antacids may be aluminum, magnesium, or calcium-based. Calcium-based antacids (usually calcium carbonate), unlike other antacids, stimulate the release of gastrin from the stomach and duodenum. Gastrin is the hormone that is primarily responsible for the stimulation of acid secretion by the stomach. Therefore, the secretion of acid rebounds after the direct acid-neutralizing effect of the calcium carbonate is exhausted. The rebound is due to the release of gastrin, which results in an overproduction of acid. Theoretically at least, this increased acid is not good for GERD.
Acid rebound, however, is not clinically important. That is, treatment with calcium carbonate is not less effective or safe than treatment with antacids not containing calcium carbonate. Nevertheless, the phenomenon of acid rebound is theoretically harmful. In practice, therefore, calcium-containing antacids such as Tums and Rolaids are not recommended for frequent use. The occasional use of these calcium carbonate-containing antacids, however, is not believed to be harmful. The advantages of calcium carbonate-containing antacids are their low cost, the calcium they add to the diet, and their convenience as compared to liquids.
Aluminum-containing antacids tend to cause constipation, while magnesium-containing antacids tend to cause diarrhea. If diarrhea or constipation becomes a problem, it may be necessary to switch antacids, or use antacids containing both aluminum and magnesium.
Although antacids can neutralize acid, they do so for only a short period. For substantial neutralization of acid throughout the day, antacids would need to be given frequently, at least every hour.
The first medication developed for the more effective and convenient treatment of acid-related diseases, including GERD, was a histamine antagonist, specifically cimetidine (Tagamet). Histamine is an important chemical because it stimulates acid production by the stomach. Released within the wall of the stomach, histamine attaches to receptors (binders) on the stomach's acid-producing cells and stimulates the cells to produce acid. Histamine antagonists work by blocking the receptor for histamine and thereby preventing histamine from stimulating the acid-producing cells. (Histamine antagonists are referred to as H2 antagonists because the specific receptor they block is the histamine type 2 receptor.)
As histamine is particularly important for the stimulation of acid after meals, H2 antagonists are best taken 30 minutes before meals. The reason for this timing is so that the H2 antagonists will be at peak levels in the body after the meal when the stomach is actively producing acid. H2 antagonists also can be taken at bedtime to suppress the nighttime production of acid.
H2 antagonists are very good for relieving the symptoms of GERD, particularly heartburn. However, they are not very good for healing the inflammation (esophagitis) that may accompany GERD. They are used primarily for the treatment of heartburn in GERD that is not associated with inflammation or complications, such as erosions or ulcers, strictures, or Barrett's esophagus.
Three different H2 antagonists are available by prescription, including cimetidine (Tagamet), nizatidine (Axid), and famotidine (Pepcid). Two of these, cimetidine (Tagamet HB) and famotidine (Pepcid AC, Zantac 360) are available over-the-counter (OTC), without the need for a prescription. However, the OTC dosages are lower than those available by prescription.
The second type of drug developed specifically for acid-related diseases, such as GERD, was a proton pump inhibitor (PPI), specifically, omeprazole (Prilosec). A PPI blocks the secretion of acid into the stomach by the acid-secreting cells. The advantage of a PPI over an H2 antagonist is that the PPI shuts off acid production more completely and for a longer period of time. Not only is the PPI good for treating the symptom of heartburn, but it also is good for protecting the esophagus from acid so that esophageal inflammation can heal.
PPIs are used when H2 antagonists do not relieve symptoms adequately or when complications of GERD such as erosions or ulcers, strictures, or Barrett's esophagus exist. Five different PPIs are approved for the treatment of GERD, including omeprazole (Prilosec, Dexilant), lansoprazole (Prevacid), rabeprazole (Aciphex), pantoprazole (Protonix), and esomeprazole (Nexium), and dexlansoprazole (Dexilant). A sixth PPI product consists of a combination of omeprazole and sodium bicarbonate (Zegerid). PPIs (except for Zegerid) are best taken an hour before meals. The reason for this timing is that the PPIs work best when the stomach is most actively producing acid, which occurs after meals. If the PPI is taken before the meal, it is at peak levels in the body after the meal when the acid is being made.
Pro-motility drugs work by stimulating the muscles of the gastrointestinal tract, including the esophagus, stomach, small intestine, and/or colon. One pro-motility drug, metoclopramide (Reglan), is approved for GERD. Pro-motility drugs increase the pressure in the lower esophageal sphincter and strengthen the contractions (peristalsis) of the esophagus. Both effects would be expected to reduce the reflux of acid. However, these effects on the sphincter and esophagus are small. Therefore, it is believed that the primary effect of metoclopramide may be to speed up emptying of the stomach, which also would be expected to reduce reflux.
Pro-motility drugs are most effective when taken 30 minutes before meals and again at bedtime. They are not very effective for treating either the symptoms or complications of GERD. Therefore, the pro-motility agents are reserved either for patients who do not respond to other treatments or are added to enhance other treatments for GERD.
Foam barriers provide a unique form of treatment for GERD. Foam barriers are tablets that are composed of an antacid and a foaming agent. As the tablet disintegrates and reaches the stomach, it turns into foam that floats on top of the liquid contents of the stomach. The foam forms a physical barrier to the reflux of liquid. At the same time, the antacid bound to the foam neutralizes acid that comes into contact with the foam. The tablets are best taken after meals (when the stomach is distended) and when lying down, both times when reflux is more likely to occur. Foam barriers are not often used as the first or only treatment for GERD. Rather, they are added to other drugs for GERD when the other drugs are not adequately effective in relieving symptoms. There is only one foam barrier, which is a combination of aluminum hydroxide gel, magnesium trisilicate, and alginate (Gaviscon).
The drugs described above usually are effective in treating the symptoms and complications of GERD. Nevertheless, sometimes they are not. For example, despite adequate suppression of acid and relief from heartburn, regurgitation, with its potential for complications in the lungs, may still occur. Moreover, the amounts and/or numbers of drugs that are required for satisfactory treatment are sometimes so great that drug treatment is unreasonable. In such situations, surgery can effectively stop reflux.
The surgical procedure that is done to prevent reflux is technically known as fundoplication and is called reflux surgery or anti-reflux surgery. During fundoplication, any hiatal hernial sac is pulled below the diaphragm and stitched there. In addition, the opening in the diaphragm through which the esophagus passes is tightened around the esophagus. Finally, the upper part of the stomach next to the opening of the esophagus into the stomach is wrapped around the lower esophagus to make an artificial lower esophageal sphincter. All of this surgery can be done through an incision in the abdomen (laparotomy) or using a technique called laparoscopy. During laparoscopy, a small viewing device and surgical instruments are passed through several small puncture sites in the abdomen. This procedure avoids the need for a major abdominal incision.
Surgery is very effective at relieving symptoms and treating the complications of GERD. Approximately 80% of patients will have good or excellent relief of their symptoms for at least 5 to 10 years. Nevertheless, many patients who have had surgery will continue to take drugs for reflux. It is not clear whether they take the drugs because they continue to have reflux and symptoms of reflux or if they take them for symptoms that are being caused by problems other than GERD. The most common complication of fundoplication is swallowed food that sticks at the artificial sphincter. Fortunately, the sticking usually is temporary. If it is not transient, endoscopic treatment to stretch (dilate) the artificial sphincter usually will relieve the problem. Only occasionally is it necessary to re-operate to revise the prior surgery.
Very recently, endoscopic techniques for the treatment of GERD have been developed and tested. One type of endoscopic treatment involves suturing (stitching) the area of the lower esophageal sphincter, which essentially tightens the sphincter.
A second type involves the application of radio-frequency waves to the lower part of the esophagus just above the sphincter. The waves cause damage to the tissue beneath the esophageal lining and a scar (fibrosis) forms. The scar shrinks and pulls on the surrounding tissue, thereby tightening the sphincter and the area above it.
A third type of endoscopic treatment involves the injection of materials into the esophageal wall in the area of the LES. The injected material is intended to increase pressure in the LES and thereby prevent reflux. In one treatment the injected material was a polymer. Unfortunately, the injection of polymer led to serious complications, and the material for injection is no longer available. Another treatment involving injection of expandable pellets also was discontinued. Limited information is available about a third type of injection which uses gelatinous polymethylmethacrylate microspheres.
Endoscopic treatment has the advantage of not requiring surgery. It can be performed without hospitalization. Experience with endoscopic techniques is limited. It is not clear how effective they are, especially long-term. Because the effectiveness and the full extent of potential complications of endoscopic techniques are not clear, it is felt generally that endoscopic treatment should only be done as part of experimental trials.
Transient LES relaxations appear to be the most common way in which acid reflux occurs. Although there is an available drug that prevents relaxations (baclofen), it has side effects that are too frequent to be generally useful. Much attention is being directed at the development of drugs that prevent these relaxations without accompanying side effects.
There are several ways to approach the evaluation and management of GERD. The approach depends primarily on the frequency and severity of symptoms, the adequacy of the response to treatment, and the presence of complications.
For infrequent heartburn, the most common symptom of GERD, life-style changes and an occasional antacid may be all that is necessary. If heartburn is frequent, daily non-prescription-strength (over-the-counter) H2 antagonists may be adequate. A foam barrier also can be used with the antacid or H2 antagonist.
If life-style changes and antacids, non-prescription H2 antagonists, and a foam barrier do not adequately relieve heartburn, it is time to see a physician for further evaluation and to consider prescription-strength drugs. The evaluation by the physician should include an assessment for possible complications of GERD based on the presence of such symptoms or findings as:
Clues to the presence of diseases that may mimic GERD, such as gastric or duodenal ulcers and esophageal motility disorders, should be sought.
If there are no symptoms or signs of complications and no suspicion of other diseases, a therapeutic trial of acid suppression with H2 antagonists often is used. If H2 antagonists are not adequately effective, a second trial, with the more potent PPIs, can be given. Sometimes, a trial of treatment begins with a PPI and skips the H2 antagonist. If treatment relieves the symptoms completely, no further evaluation may be necessary and the effective drug, the H2 antagonist or PPI, is continued. As discussed previously, however, there are potential problems with this commonly used approach, and some physicians would recommend a further evaluation for almost all patients they see.
If at the time of evaluation, there are symptoms or signs that suggest complicated GERD or a disease other than GERD or if the relief of symptoms with H2 antagonists or PPIs is not satisfactory, a further evaluation by endoscopy (EGD) definitely should be done.
There are several possible results of endoscopy and each requires a different approach to treatment. If the esophagus is normal and no other diseases are found, the goal of treatment simply is to relieve symptoms. Therefore, prescription strength H2 antagonists or PPIs are appropriate. If damage to the esophagus (esophagitis or ulceration) is found, the goal of treatment is healing the damage. In this case, PPIs are preferred over H2 antagonists because they are more effective for healing.
If complications of GERD, such as stricture or Barrett's esophagus are found, treatment with PPIs also is more appropriate. However, the adequacy of the PPI treatment probably should be evaluated with a 24-hour pH study during treatment with the PPI. (With PPIs, although the amount of acid reflux may be reduced enough to control symptoms, it may still be abnormally high. Therefore, judging the adequacy of suppression of acid reflux by only the response of symptoms to treatment is not satisfactory.) Strictures may also need to be treated by endoscopic dilatation (widening) of the esophageal narrowing. With Barrett's esophagus, periodic endoscopic examination should be done to identify pre-malignant changes in the esophagus.
If symptoms of GERD do not respond to maximum doses of PPI, there are two options for management. The first is to perform 24-hour pH testing to determine whether the PPI is ineffective or if a disease other than GERD is likely to be present. If the PPI is ineffective, a higher dose of PPI may be tried. The second option is to go ahead without 24 hour pH testing and to increase the dose of PPI. Another alternative is to add another drug to the PPI that works in a way that is different from the PPI, for example, a pro-motility drug or a foam barrier. If necessary, all three types of drugs can be used. If there is not a satisfactory response to this maximal treatment, 24 hour pH testing should be done.
Who should consider surgery or, perhaps, an endoscopic treatment trial for GERD? (As mentioned previously, the effectiveness of the recently developed endoscopic treatments remains to be determined.) Patients should consider surgery if they have regurgitation that cannot be controlled with drugs. This recommendation is particularly important if the regurgitation results in infections in the lungs or occurs at night when aspiration into the lungs is more likely. Patients also should consider surgery if they require large doses of PPI or multiple drugs to control their reflux. It is debated whether or not a desire to be free of the need to take life-long drugs to prevent symptoms of GERD is by itself a satisfactory reason for having surgery.
Some physicians - primarily surgeons - recommend that all patients with Barrett's esophagus should have surgery. This recommendation is based on the belief that surgery is more effective than endoscopic surveillance or ablation of the abnormal tissue followed by treatment with acid-suppressing drugs in preventing both the reflux and the cancerous changes in the esophagus. There are no studies, however, demonstrating the superiority of surgery over drugs or ablation for the treatment of GERD and its complications. Moreover, the effectiveness of drug treatment can be monitored with 24 hour pH testing.
One unresolved issue in GERD is the inconsistent relationships among acid reflux, heartburn, and damage to the lining of the esophagus (esophagitis and the complications).
Clearly, we have much to learn about the relationship between acid reflux and esophageal damage, and about the processes (mechanisms) responsible for heartburn. This issue is of more than passing interest. Knowledge of the mechanisms that produce heartburn and esophageal damage raises the possibility of new treatments that would target processes other than acid reflux.
One of the more interesting theories that has been proposed to answer some of these questions involves the reason for pain when acid refluxes. It often is assumed that the pain is caused by irritating acid contacting an inflamed esophageal lining. But the esophageal lining usually is not inflamed. It is possible therefore, that the acid is stimulating the pain nerves within the esophageal wall just beneath the lining. Although this may be the case, a second explanation is supported by the work of one group of scientists. These scientists find that heartburn provoked by acid in the esophagus is associated with contraction of the muscle in the lower esophagus. Perhaps it is the contraction of the muscle that somehow leads to the pain. It also is possible, however, that the contraction is an epiphenomenon, that is, refluxed acid stimulates pain nerves and causes the muscle to contract, but it is not the contraction that causes the pain. More studies will be necessary before the exact mechanism(s) that causes heartburn is clear.
There are potentially injurious agents that can be refluxed other than acid, for example, bile. Until recently it has been impossible or difficult to accurately identify non-acid reflux and, therefore, to study whether or not non-acid reflux is injurious or can cause symptoms.
A new technology allows the accurate determination of non-acid reflux. This technology uses the measurement of impedance changes within the esophagus to identify reflux of liquid, be it acid or non-acid. By combining measurement of impedance and pH it is possible to identify reflux and to tell if the reflux is acid or non-acid. It is too early to know how important non-acid reflux is in causing esophageal damage, symptoms, or complications, but there is little doubt that this new technology will be able to resolve the issues surrounding non-acid reflux.
 Prípadová štúdia:Montse si lieči deravé črevo
Preskakovanie z diéty na diétu v nádeji, že nájdeme tú magickú, je pravdepodobne niečo, čo už niekedy zažil každý z nás. Pravdou je, že neexistuje žiadna zázračná diéta, tak veľmi, ako som chcel, aby
Prípadová štúdia:Montse si lieči deravé črevo
Preskakovanie z diéty na diétu v nádeji, že nájdeme tú magickú, je pravdepodobne niečo, čo už niekedy zažil každý z nás. Pravdou je, že neexistuje žiadna zázračná diéta, tak veľmi, ako som chcel, aby
 Káva pomáha vyvíjať zdravé črevné mikróby a napomáha pohybom čriev
Existuje neoficiálny dôkaz, že konzumenti kávy prisahajú na svoju rannú šálku na bežné ranné pohyby čriev. Nová štúdia výskumníkov z Texasu ukázala, že káva skutočne pomáha pri vyprázdňovaní a zlepšuj
Káva pomáha vyvíjať zdravé črevné mikróby a napomáha pohybom čriev
Existuje neoficiálny dôkaz, že konzumenti kávy prisahajú na svoju rannú šálku na bežné ranné pohyby čriev. Nová štúdia výskumníkov z Texasu ukázala, že káva skutočne pomáha pri vyprázdňovaní a zlepšuj
 Čo jesť, keď máte GERD
Diéta pri gastroezofageálnej refluxnej chorobe (GERD) je dôležitou súčasťou liečby GERD, čo je chronický stav. Je tiež užitočný pri občasnom pálení záhy (známy aj ako reflux kyseliny). Diéta sa zame
Čo jesť, keď máte GERD
Diéta pri gastroezofageálnej refluxnej chorobe (GERD) je dôležitou súčasťou liečby GERD, čo je chronický stav. Je tiež užitočný pri občasnom pálení záhy (známy aj ako reflux kyseliny). Diéta sa zame