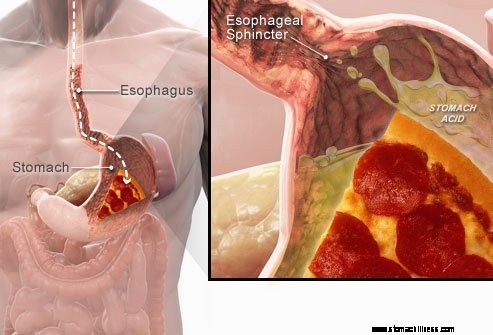
 Kai ryjate maistą, jis keliauja stemple ir eina per raumenų žiedą, vadinamą apatiniu stemplės sfinkteriu ( LES). Ši struktūra atsidaro, kad maistas galėtų patekti į skrandį. Jis turėtų likti uždarytas, kad skrandžio turinys liktų ten, kur jis priklauso.
Kai ryjate maistą, jis keliauja stemple ir eina per raumenų žiedą, vadinamą apatiniu stemplės sfinkteriu ( LES). Ši struktūra atsidaro, kad maistas galėtų patekti į skrandį. Jis turėtų likti uždarytas, kad skrandžio turinys liktų ten, kur jis priklauso.
GERL arba rūgšties refliukso simptomus sukelia rūgštaus skysto skrandžio turinio atpylimas atgal į stemplę. Dažniausias GERL simptomas yra rėmuo.
Kiti simptomai, kurie gali atsirasti dėl GERL, yra šie:
 Dažniausias GERL simptomas yra rėmuo.
Dažniausias GERL simptomas yra rėmuo. Gastroezofaginio refliukso liga, paprastai vadinama GERL arba rūgšties refliuksu, yra būklė, kai skystis skrandyje regurgituoja (atsitraukia arba grįžta) į stemplę. Skystis gali uždegti ir pažeisti gleivinę (ezofagitą), nors matomi uždegimo požymiai pasireiškia nedaugeliui pacientų. Regurgituotame skystyje paprastai yra rūgšties ir pepsino, kuriuos gamina skrandis. (Pepsinas yra fermentas, kuris pradeda baltymų virškinimą skrandyje.) Refluksuojamame skystyje taip pat gali būti tulžies, kuri iš dvylikapirštės žarnos pateko į skrandį. Pirmoji plonosios žarnos dalis, pritvirtinta prie skrandžio. Manoma, kad rūgštis yra žalingiausia grįžtamojo skysčio sudedamoji dalis. Pepsinas ir tulžis taip pat gali pažeisti stemplę, tačiau jų vaidmuo stemplės uždegimo ir pažeidimo procese nėra toks aiškus kaip rūgšties vaidmuo.
GERL yra lėtinė liga. Kai jis prasideda, jis paprastai trunka visą gyvenimą. Jei yra stemplės gleivinės pažeidimas (ezofagitas), tai taip pat yra lėtinė būklė. Be to, gydant stemplę sugijus ir nutraukus gydymą, daugumai pacientų sužalojimas atsinaujins per kelis mėnesius. Pradėjus gydyti GERL, jį reikės tęsti neribotą laiką. Tačiau kai kurie pacientai, kuriems pasireiškia periodiniai simptomai ir neserga ezofagitu, gali būti gydomi tik simptominiais laikotarpiais.
Tiesą sakant, skysto skrandžio turinio refliuksas į stemplę pasireiškia daugeliui normalių žmonių. Vienas tyrimas parodė, kad refliuksas dažnai pasireiškia normaliems žmonėms, kaip ir pacientams, sergantiems GERL. Tačiau pacientams, sergantiems GERL, grįžtamame skystyje dažniau būna rūgšties, o rūgštis ilgiau išlieka stemplėje. Taip pat buvo nustatyta, kad pacientams, sergantiems GERL, skysčių refliuksas stemplėje yra didesnis nei normalių asmenų.
Kaip dažnai būna, organizmas turi būdų apsisaugoti nuo žalingo refliukso ir rūgšties poveikio. Pavyzdžiui, dažniausiai refliuksas pasireiškia per dieną, kai asmenys yra vertikaliai. Vertikalioje padėtyje grįžtamasis skystis dėl gravitacijos greičiausiai nutekės atgal į skrandį. Be to, būdami pabudę, jie nuolat ryja, neatsižvelgiant į tai, ar yra refliuksas, ar ne. Kiekviena kregždė neša bet kokį grįžtamą skystį atgal į skrandį. Galiausiai seilių liaukos burnoje gamina seiles, kuriose yra bikarbonato. Kiekvieną kartą nurijus, bikarbonato turinčios seilės keliauja žemyn stemple. Bikarbonatas neutralizuoja nedidelį kiekį rūgšties, kuri lieka stemplėje po to, kai gravitacija ir nurijus pašalino didžiąją dalį rūgštinio skysčio.
Gravitacija, rijimas ir seilės yra svarbūs stemplės apsaugos mechanizmai, tačiau jie veiksmingi tik tada, kai asmenys yra vertikalioje padėtyje. Naktį miegant gravitacija neveikia, nustoja rijimas, sumažėja seilių išsiskyrimas. Todėl dėl refliukso, atsirandančio naktį, rūgštis ilgiau išliks stemplėje ir dar labiau pažeis stemplę.
Dėl tam tikrų sąlygų asmuo tampa jautrus GERL. Pavyzdžiui, GERL gali būti rimta problema nėštumo metu. Padidėjęs hormonų kiekis nėštumo metu tikriausiai sukelia refliuksą, nes sumažėja slėgis apatiniame stemplės sfinkteryje (žr. toliau). Tuo pačiu metu augantis vaisius padidina spaudimą pilve. Tikimasi, kad abu šie poveikiai padidins refliuksą. Taip pat pacientams, sergantiems ligomis, dėl kurių susilpnėja stemplės raumenys, pvz., sklerodermija ar mišriomis jungiamojo audinio ligomis, dažniau išsivysto GERL.
GERL priežastis yra sudėtinga ir gali turėti daug priežasčių. Be to, skirtingos priežastys gali turėti įtakos skirtingiems asmenims ar net tam pačiam asmeniui skirtingu metu. Nedidelis skaičius pacientų, sergančių GERL, gamina neįprastai daug rūgšties, tačiau tai yra neįprasta ir nėra prisidedantis prie daugelio pacientų.
Veiksniai, prisidedantys prie GERL, yra:
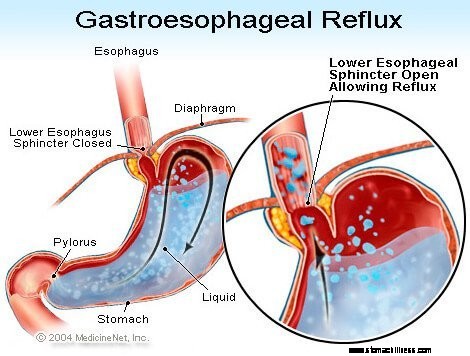
Apatinio stemplės sfinkterio (LES) veikimas yra bene svarbiausias veiksnys (mechanizmas), užkertantis kelią refliuksui. Stemplė yra raumeningas vamzdelis, besitęsiantis nuo apatinės gerklės dalies iki skrandžio. LES yra specializuotas raumenų žiedas, supantis žemiausią stemplės galą, kur jis jungiasi su skrandžiu. Raumenys, sudarantys LES, yra aktyvūs didžiąją laiko dalį, ty ramybės būsenoje. Tai reiškia, kad jis susitraukia ir uždaro praėjimą iš stemplės į skrandį. Šis kanalo uždarymas apsaugo nuo refliukso. Nurijus maistą ar seilę, LES atsipalaiduoja kelioms sekundėms, kad maistas ar seilės galėtų patekti iš stemplės į skrandį, o tada vėl užsidaro.
Pacientams, sergantiems GERL, buvo nustatyta keletas skirtingų LES anomalijų. Du iš jų susiję su LES funkcija. Pirmasis yra neįprastai silpnas LES susitraukimas, dėl kurio sumažėja jo gebėjimas užkirsti kelią refliuksui. Antrasis yra nenormalus LES atsipalaidavimas, vadinamas trumpalaikiu LES atsipalaidavimu. Jie nenormalūs tuo, kad nelydi kregždžių ir laikosi ilgai, iki kelių minučių. Šie užsitęsę atsipalaidavimai leidžia lengviau atsirasti refliuksui. Laikini LES atsipalaidavimai pasireiškia pacientams, sergantiems GERL, dažniausiai po valgio, kai skrandis yra išsipūtęs su maistu. Laikini LES atsipalaidavimai taip pat pasitaiko asmenims, neturintiems GERL, tačiau jie yra nedažni.
Neseniai aprašyta GERL sergančių pacientų anomalija yra LES laisvumas. Konkrečiai, panašus išsipūtimo slėgis labiau atveria LES pacientams, sergantiems GERL, nei asmenims, neturintiems GERL. Bent jau teoriškai tai leistų lengviau atidaryti LES ir (arba) padidinti rūgšties srautą atgal į stemplę, kai LES yra atidaryta.
Hiatal išvaržos prisideda prie refliukso, nors būdas, kaip jos prisideda, nėra aiškus. Daugumai pacientų, sergančių GERL, yra išvaržų, tačiau daugelis jų neturi. Todėl norint susirgti GERL nebūtina turėti hiatalinę išvaržą. Be to, daugelis žmonių turi hiatalinių išvaržų, bet neserga GERL. Nėra tiksliai žinoma, kaip ir kodėl vystosi hiatalinės išvaržos.
Paprastai LES yra tame pačiame lygyje, kur stemplė eina iš krūtinės per nedidelę angą diafragmoje ir į pilvą. (Diafragma yra raumeninga, horizontali pertvara, skirianti krūtinę nuo pilvo.) Kai yra hiatalinė išvarža, nedidelė viršutinės skrandžio dalies dalis, kuri prisitvirtina prie stemplės, stumiasi aukštyn per diafragmą. Dėl to nedidelė skrandžio dalis ir LES patenka į krūtinę, o LES nebėra diafragmos lygyje.
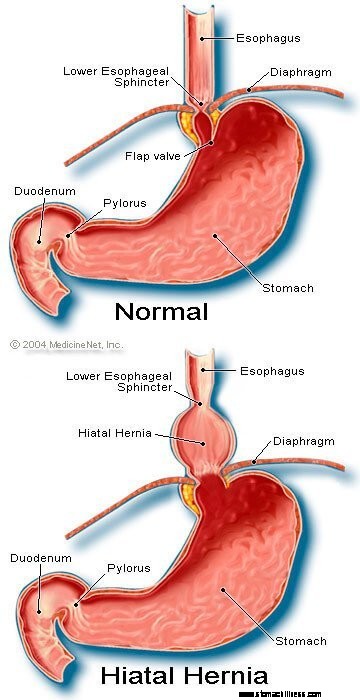 Hiatal išvaržos vaizdas
Hiatal išvaržos vaizdas
Atrodo, kad diafragma, kuri supa LES, yra svarbi siekiant užkirsti kelią refliuksui. Tai reiškia, kad asmenims, neturintiems hiatalinių išvaržų, stemplę supanti diafragma nuolat susitraukia, bet tada atsipalaiduoja nuryjant, kaip ir LES. Atkreipkite dėmesį, kad LES ir diafragmos poveikis pasireiškia toje pačioje vietoje pacientams, kuriems nėra hiatal išvaržų. Todėl refliukso barjeras yra lygus LES ir diafragmos sukuriamų slėgių sumai. Kai LES juda į krūtinę su hiatal išvarža, diafragma ir LES toliau daro spaudimą ir barjerinį poveikį. Tačiau dabar jie tai daro skirtingose vietose. Todėl slėgis nebėra adityvus. Vietoj to, vienas aukšto slėgio barjeras refliuksui pakeičiamas dviem mažesnio slėgio barjerais, todėl refliuksas atsiranda lengviau. Taigi, slėgio barjero mažinimas yra vienas iš būdų, kaip hiatal išvarža gali prisidėti prie refliukso.
Kaip minėta anksčiau, kregždės yra svarbios pašalinant rūgštį iš stemplės. Prarijus sukelia žiedą primenančią stemplės raumenų susitraukimo bangą, kuri susiaurina stemplės spindį (vidinę ertmę). Susitraukimas, vadinamas peristaltika, prasideda viršutinėje stemplės dalyje ir keliauja į apatinę stemplę. Jis stumia maistą, seiles ir visa, kas yra stemplėje, į skrandį.
Kai susitraukimo banga yra netinkama, refliukso rūgštis nėra stumiama atgal į skrandį. Pacientams, sergantiems GERL, aprašyti keli susitraukimo sutrikimai. Pavyzdžiui, susitraukimo bangos gali neprasidėti po kiekvieno rijimo arba susitraukimo bangos gali išnykti nepasiekusios skrandžio. Be to, susitraukimų sukuriamas slėgis gali būti per silpnas, kad rūgštis būtų sugrąžinta į skrandį. Tokie susitraukimų sutrikimai, dėl kurių sumažėja rūgšties pašalinimas iš stemplės, dažnai nustatomi pacientams, sergantiems GERL. Tiesą sakant, jie dažniausiai nustatomi tiems pacientams, kuriems yra sunkiausia GERL. Tikimasi, kad nenormalių stemplės susitraukimų poveikis bus blogesnis naktį, kai gravitacija nepadeda grąžinti refliuksinės rūgšties į skrandį. Atkreipkite dėmesį, kad rūkymas taip pat žymiai sumažina rūgšties pašalinimą iš stemplės. Šis poveikis išlieka mažiausiai 6 valandas po paskutinės cigaretės.
Dažniausiai refliuksas per dieną pasireiškia po valgio. Šis refliuksas tikriausiai atsirado dėl trumpalaikio LES atsipalaidavimo, kurį sukelia skrandžio išsipūtimas su maistu. Maždaug mažumos pacientų, sergančių GERL, skrandis po valgio tuštinasi neįprastai lėtai. Tai vadinama gastropareze. Lėtesnis skrandžio ištuštinimas pailgina skrandžio išsipūtimą su maistu po valgio. Todėl lėtesnis ištuštinimas pailgina laikotarpį, per kurį didesnė refliukso tikimybė. Yra keletas vaistų, susijusių su skrandžio ištuštinimo sutrikimu, pavyzdžiui:
Asmenys neturėtų nustoti vartoti šių ar kitų išrašytų vaistų, kol juos išrašęs gydytojas neaptarė su jais galimos GERL situacijos.
Nekomplikuoto GERL simptomai pirmiausia yra:
Kiti simptomai atsiranda, kai yra GERL komplikacijų, ir jie bus aptarti su komplikacijomis.
Kai GERL sergančių pacientų rūgštis grįžta atgal į stemplę, stimuliuojamos nervinės skaidulos stemplėje. Ši nervų stimuliacija dažniausiai sukelia rėmenį, skausmą, būdingą GERL. Rėmuo paprastai apibūdinamas kaip deginantis skausmas krūtinės viduryje. Jis gali prasidėti nuo pilvo arba gali prasidėti iki kaklo. Tačiau kai kuriems pacientams skausmas gali būti aštrus arba panašus į spaudimą, o ne deginantis. Toks skausmas gali būti panašus į širdies skausmą (krūtinės anginą). Kitiems pacientams skausmas gali plisti į nugarą.
Kadangi rūgšties refliuksas yra dažnesnis po valgio, rėmuo dažniau pasireiškia po valgio. Rėmuo taip pat dažniau pasireiškia gulint, nes be gravitacijos poveikio refliuksas atsiranda lengviau, rūgštis grįžta į skrandį lėčiau. Daugelį pacientų, sergančių GERL, iš miego pažadina rėmuo.
Rėmens epizodai dažniausiai pasitaiko periodiškai. Tai reiškia, kad epizodai yra dažnesni arba sunkesni kelias savaites ar mėnesius, o vėliau retėja arba sunkūs arba net išnyksta kelias savaites ar mėnesius. Toks simptomų periodiškumas suteikia pagrindą pacientams, sergantiems GERL, nesergantiems ezofagitu, gydyti su pertraukomis. Nepaisant to, rėmuo yra visą gyvenimą trunkanti problema ir beveik visada atsinaujina.
Regurgitacija – tai skysčių su refliuksu atsiradimas burnoje. Daugumai pacientų, sergančių GERL, į stemplę paprastai patenka tik nedidelis skysčio kiekis, o skystis lieka apatinėje stemplės dalyje. Retkarčiais kai kuriems pacientams, sergantiems GERL, didesni skysčių kiekiai, kartais kurių sudėtyje yra maisto, sukelia refliuksą ir pasiekia viršutinę stemplę.
Viršutiniame stemplės gale yra viršutinis stemplės sfinkteris (UES). UES yra apskritas raumenų žiedas, kuris savo veiksmais labai panašus į LES. Tai reiškia, kad UES neleidžia stemplės turiniui patekti į gerklę. Kai nedidelis kiekis grįžtamojo skysčio ir (arba) maisto patenka pro UES ir patenka į gerklę, burnoje gali būti rūgštus skonis. Jei didesni kiekiai pažeidžia UES, pacientai gali staiga pastebėti, kad jų burna prisipildo skysčio ar maisto. Be to, dažnas ar užsitęsęs regurgitacija gali sukelti rūgšties sukeltą dantų eroziją.
Pykinimas sergant GERL yra nedažnas. Tačiau kai kuriems pacientams jis gali būti dažnas arba sunkus ir gali sukelti vėmimą. Tiesą sakant, pacientams, kuriems yra nepaaiškinamas pykinimas ir (arba) vėmimas, GERL yra viena iš pirmųjų būklių, į kurią reikia atsižvelgti. Neaišku, kodėl kai kuriems GERL sergantiems pacientams dažniausiai pasireiškia rėmuo, o kitiems – pykinimas.
Skystis iš skrandžio, grįžtantis į stemplę, pažeidžia stemplę dengiančias ląsteles. Kūnas reaguoja taip, kaip paprastai reaguoja į žalą, kuri yra uždegimu (ezofagitu). Uždegimo tikslas yra neutralizuoti žalingą agentą ir pradėti gijimo procesą. Jei pažeidimas giliai patenka į stemplę, susidaro opa. Opa yra tiesiog stemplės gleivinės plyšimas, atsirandantis uždegimo srityje. Opos ir jų sukeliamas papildomas uždegimas gali įsiskverbti į stemplės kraujagysles ir sukelti kraujavimą į stemplę.
Kartais kraujavimas yra stiprus ir gali prireikti:
Stemplės opos gyja susidarant randams (fibrozei). Laikui bėgant randinis audinys susitraukia ir susiaurina stemplės spindį (vidinę ertmę). Šis randuotas susiaurėjimas vadinamas striktūra. Prarijus maistas gali įstrigti stemplėje, kai susiaurėjimas tampa pakankamai stiprus (dažniausiai kai jis apriboja stemplės spindį iki vieno centimetro skersmens). Dėl šios situacijos gali prireikti endoskopiškai pašalinti įstrigusį maistą. Tada, kad maistas nepriliptų, susiaurėjimą reikia ištempti (paplatinti). Be to, norint išvengti striktūros pasikartojimo, taip pat reikia užkirsti kelią refliuksui.
Ilgalaikis ir (arba) sunkus GERL kai kuriems pacientams sukelia pokyčius ląstelėse, kurios iškloja stemplę. Šios ląstelės yra ikivėžinės ir, nors paprastai, gali tapti vėžinėmis. Ši būklė vadinama Bareto stemple ir pasireiškia maždaug 10% pacientų, sergančių GERL. Stemplės vėžio tipas, susijęs su Bareto stemple (adenokarcinoma), dažnėja. Neaišku, kodėl kai kuriems pacientams, sergantiems GERL, išsivysto Bareto stemplė, tačiau daugumai jų nepasireiškia.
Bareto stemplę galima vizualiai atpažinti endoskopijos metu ir patvirtinti mikroskopu ištyrus gleivinės ląsteles. Tada pacientams, sergantiems Bareto stemple, gali būti periodiškai atliekamos stebėjimo endoskopijos ir biopsijos, nors nesutariama, kuriuos pacientus reikia stebėti. Stebėjimo tikslas – nustatyti progresavimą nuo ikivėžinių pokyčių iki vėžinių pokyčių, kad būtų galima pradėti vėžio prevencinį gydymą. Taip pat manoma, kad pacientai, sergantys Bareto stemple, turėtų gauti maksimalų GERL gydymą, kad būtų išvengta tolesnio stemplės pažeidimo. Tiriamos procedūros, kuriomis pašalinamos nenormalios gleivinės ląstelės. Ląstelėms pašalinti gali būti naudojami keli endoskopiniai nechirurginiai metodai. Šie metodai yra patrauklūs, nes jiems nereikia operacijos; tačiau yra susijusių su komplikacijų, o ilgalaikis gydymo veiksmingumas dar nenustatytas. Chirurginis stemplės pašalinimas visada yra galimybė.
Daugelis nervų yra apatinėje stemplės dalyje. Kai kuriuos iš šių nervų stimuliuoja refliukso rūgštis, o tai sukelia skausmą (dažniausiai rėmenį). Kiti stimuliuojami nervai nesukelia skausmo. Vietoj to, jie stimuliuoja dar kitus nervus, kurie provokuoja kosulį. Tokiu būdu grįžtamasis skystis gali sukelti kosulį, nepasiekdamas gerklės! Panašiai refliuksas į apatinę stemplę gali stimuliuoti stemplės nervus, kurie jungiasi ir gali stimuliuoti nervus, einančius į plaučius. Dėl šių plaučių nervų mažesni kvėpavimo vamzdeliai gali susiaurėti ir sukelti astmos priepuolį.
Nors GERL gali sukelti kosulį, tai nėra dažna nepaaiškinamo kosulio priežastis. Nors GERL taip pat gali būti astmos priežastis, labiau tikėtina, kad ji sukelia astmos priepuolius pacientams, kurie jau serga astma. Nors lėtinis kosulys ir astma yra dažni negalavimai, neaišku, kaip dažnai juos pasunkina ar sukelia GERL.
Jei grįžtamasis skystis patenka pro viršutinį stemplės sfinkterį, jis gali patekti į gerklę (ryklę) ir net į balso dėžutę (gerklą). Atsiradęs uždegimas gali sukelti gerklės skausmą ir užkimimą. Kaip ir sergant kosuliu ir astma, neaišku, kaip dažnai GERL sukelia kitaip nepaaiškinamą gerklės ir gerklų uždegimą.
Refluksuojantis skystis, kuris patenka iš gerklės (ryklės) ir patenka į gerklas, gali patekti į plaučius (aspiracija). Skysčio refliuksas į plaučius (vadinamas aspiracija) dažnai sukelia kosulį ir užspringimą. Tačiau aspiracija taip pat gali pasireikšti nesukeliant šių simptomų. Su šiais simptomais arba be jų, aspiracija gali sukelti plaučių infekciją ir sukelti plaučių uždegimą. Šio tipo pneumonija yra rimta problema, kurią reikia nedelsiant gydyti. Kai aspiraciją lydi simptomai, gali atsirasti lėtas, progresuojantis plaučių randėjimas (plaučių fibrozė), kuris gali būti matomas krūtinės ląstos rentgenogramose. Aspiracija dažniau pasireiškia naktį, nes tada neaktyvūs procesai (mechanizmai), apsaugantys nuo refliukso, o plaučius saugantis kosulio refleksas taip pat neaktyvus.
Gerklė bendrauja su nosies kanalais. Mažiems vaikams du limfinio audinio lopai, vadinami adenoidais, yra ten, kur viršutinė gerklės dalis jungiasi su nosies kanalais. Iš sinusų kanalai ir vamzdeliai iš vidurinės ausies (Eustachijaus vamzdeliai) atsiveria į užpakalinius nosies kanalus šalia adenoidų. Viršutinėje gerklėje patekęs refliuksuotas skystis gali uždegti adenoidus ir sukelti jų patinimą. Tada patinę adenoidai gali užblokuoti kanalus iš sinusų ir Eustachijaus vamzdelių. Kai sinusai ir vidurinės ausys yra uždaryti nuo nosies takų dėl adenoidų patinimo, juose kaupiasi skystis. Toks skysčių kaupimasis gali sukelti diskomfortą sinusuose ir ausyse. Kadangi adenoidai yra ryškūs mažiems vaikams, o ne suaugusiems, šis skysčių kaupimasis ausyse ir sinusuose pastebimas vaikams, o ne suaugusiems.
Yra įvairių procedūrų, testų ir simptomų (pvz., rėmens) įvertinimo, kad būtų galima diagnozuoti ir įvertinti GERL sergančius pacientus.
Įprastas GERL yra būdingas simptomas, rėmuo. Rėmuo dažniausiai apibūdinamas kaip poodinis (po krūtinės viduriu) deginimas, atsirandantis pavalgius ir dažnai paūmėjantis gulint. Norėdami patvirtinti diagnozę, gydytojai dažnai gydo pacientus vaistais, slopinančiais skrandžio rūgšties gamybą. Jei rėmuo labai sumažėja, GERL diagnozė laikoma patvirtinta. Toks diagnozės nustatymo metodas, pagrįstas simptomų atsaku į gydymą, paprastai vadinamas terapiniu tyrimu.
Taikant šį metodą kyla problemų. Pavyzdžiui, pacientai, kurių būklė gali būti panaši į GERL, ypač dvylikapirštės žarnos arba skrandžio (skrandžio) opa, taip pat gali reaguoti į tokį gydymą. Esant tokiai situacijai, jei gydytojas mano, kad problema yra GERL, nepastebėta opos ligos priežastis, pvz., infekcijos tipas, vadinamas Helicobacter pylori. (H. pylori ), arba nesteroidiniai vaistai nuo uždegimo arba NVNU (pvz., ibuprofenas), taip pat gali sukelti opas, todėl šios ligos būtų gydomos kitaip nei GERL.
Be to, kaip ir bet kokio gydymo atveju, placebo efektas gali siekti 20 %, o tai reiškia, kad 20 % pacientų reaguos į placebo (neaktyvias) tabletes arba, tiesą sakant, į bet kokį gydymą. Tai reiškia, kad 20 % pacientų, kurių simptomų priežastys yra kitos nei GERL (arba opos), po gydymo nuo GERL simptomai sumažės. Taigi, remiantis jų atsaku į gydymą (terapinis tyrimas), šie pacientai ir toliau bus gydomi nuo GERL, net jei jie neserga GERL. Be to, tikroji jų simptomų priežastis nebus išaiškinta.
Viršutinės virškinimo trakto endoskopija (taip pat žinoma kaip stemplės-gastro-duodenoskopija arba EGD) yra dažnas GERL diagnozavimo būdas. EGD yra procedūra, kurios metu praryjamas vamzdelis su optine vizualizavimo sistema. Vamzdeliui einant žemyn virškinamuoju traktu, galima ištirti stemplės, skrandžio ir dvylikapirštės žarnos gleivinę.
Daugumos pacientų, kuriems pasireiškia refliukso simptomai, stemplė atrodo normali. Todėl daugumai pacientų endoskopija nepadės diagnozuoti GERL. Tačiau kartais stemplės gleivinė atrodo uždegusi (ezofagitas). Be to, jei pastebimos erozijos (paviršiniai stemplės gleivinės įtrūkimai) arba opos (gilesnės gleivinės įtrūkimai), galima patikimai diagnozuoti GERL. Endoskopija taip pat nustatys keletą GERL komplikacijų, ypač opų, susiaurėjimų ir Bareto stemplės. Taip pat gali būti paimtos biopsijos.
Galiausiai, naudojant EGD, galima diagnozuoti kitas įprastas problemas, kurios gali sukelti į GERL panašius simptomus (pvz., opos, uždegimas arba skrandžio arba dvylikapirštės žarnos vėžys).
Stemplės biopsijos, gautos naudojant endoskopą, nėra laikomos labai naudingomis diagnozuojant GERL. Tačiau jie yra naudingi diagnozuojant vėžį arba stemplės uždegimo priežastis, išskyrus rūgšties refliuksą, ypač infekcijas. Be to, biopsijos yra vienintelė priemonė diagnozuoti Bareto stemplės ląstelių pokyčius. Visai neseniai buvo pasiūlyta, kad net pacientams, sergantiems GERL, kurių stemplės akiai atrodo normalios, biopsijos parodys tarpų tarp gleivinės ląstelių išsiplėtimą, o tai gali būti pažeidimo požymis. Tačiau dar per anksti daryti išvadą, kad išplėtimas yra pakankamai konkretus, kad būtų galima įsitikinti, jog yra GERL.
Prieš pradedant endoskopiją, stemplės rentgenograma (vadinama stemple) buvo vienintelė priemonė diagnozuoti GERL. Pacientai nurijo barį (kontrastinę medžiagą), o tada buvo darytos bario užpildytos stemplės rentgeno nuotraukos. Stemplės problema buvo ta, kad tai buvo nejautrus GERL diagnozavimo testas. Tai reiškia, kad daugeliui pacientų, sirgusių GERL, nepavyko rasti GERL požymių, nes pacientai turėjo mažai arba visai nepažeidė stemplės gleivinės. Rentgeno spinduliai galėjo parodyti tik retas GERL komplikacijas, pavyzdžiui, opas ir susiaurėjimus. Rentgeno spindulių buvo atsisakyta kaip GERL diagnozavimo priemonės, nors jie vis dar gali būti naudingi kartu su endoskopija vertinant komplikacijas.
Kai GERL pažeidžia gerklę ar gerklas ir sukelia kosulio, užkimimo ar gerklės skausmo simptomus, pacientai dažnai kreipiasi į ausų, nosies ir gerklės (ENT) specialistą. ENT specialistas dažnai nustato gerklės ar gerklų uždegimo požymius. Nors dažniausiai uždegimą sukelia gerklės ar gerklų ligos, kartais priežastis gali būti GERL. Atitinkamai, ENT specialistai dažnai bando rūgštingumą slopinantį gydymą, kad patvirtintų GERL diagnozę. Tačiau šis metodas turi tas pačias problemas, kaip ir anksčiau, kurios kyla dėl atsako į gydymą panaudojimo GERL patvirtinimui.
Stemplės rūgšties tyrimas laikomas „auksiniu standartu“ diagnozuojant GERL. Kaip aptarta anksčiau, rūgšties refliuksas yra dažnas bendroje populiacijoje. Tačiau pacientams, sergantiems GERL simptomais ar komplikacijomis, refliuksas yra daugiau nei asmenims, neturintiems GERL simptomų ar komplikacijų. Be to, normalius asmenis ir pacientus, sergančius GERL, galima vidutiniškai gerai atskirti vienas nuo kito pagal laiką, per kurį stemplėje yra rūgšties.
Laikas, per kurį stemplėje yra rūgšties, nustatomas atliekant testą, vadinamą 24 valandų stemplės pH testu. (pH yra matematinis rūgštingumo kiekio išreiškimo būdas.) Šiam tyrimui per nosį įleidžiamas mažas vamzdelis (kateteris) ir įdedamas į stemplę. Ant kateterio galo yra jutiklis, kuris jaučia rūgštį. Kitas kateterio galas išeina iš nosies, apsivynioja per ausį ir nukeliauja iki juosmens, kur pritvirtinamas prie magnetofono. Kiekvieną kartą, kai rūgštis grįžta atgal į stemplę iš skrandžio, ji stimuliuoja jutiklį ir registratorius įrašo refliukso epizodą. Po 20–24 valandų kateteris pašalinamas ir registruojamas refliukso įrašas iš registratoriaus.
Yra problemų naudojant pH tyrimą diagnozuojant GERL. Nepaisant to, kad normalius asmenis ir pacientus, sergančius GERL, galima gana gerai atskirti remiantis pH tyrimais, atskyrimas nėra tobulas. Todėl kai kuriems pacientams, sergantiems GERL, rūgšties refliuksas bus normalus, o kai kuriems pacientams, nesergantiems GERL, rūgšties refliuksas bus nenormalus. Norint patvirtinti GERL buvimą, reikia ne tik pH testo, bet, pavyzdžiui, tipinių simptomų, atsako į gydymą arba GERL komplikacijų. GERL taip pat gali būti užtikrintai diagnozuotas, kai rėmens epizodai koreliuoja su rūgšties refliuksu, kaip rodo rūgšties tyrimai.
PH tyrimas yra naudingas gydant GERL ne tik diagnozuojant GERL. Pavyzdžiui, testas gali padėti nustatyti, kodėl GERL simptomai nereaguoja į gydymą. Galbūt 10–20 procentų pacientų simptomai iš esmės nepagerės gydant GERL. Tokį atsako į gydymą nebuvimą gali sukelti neveiksmingas gydymas. Tai reiškia, kad vaistas nepakankamai slopina rūgšties gamybą skrandyje ir nesumažina rūgšties refliukso. Arba atsako nebuvimas gali būti paaiškintas neteisinga GERL diagnoze. Abiem atvejais pH testas gali būti labai naudingas. Jei tyrimas atskleidžia didelį rūgšties refliuksą, kai tęsiamas gydymas, gydymas yra neveiksmingas ir jį reikės pakeisti. Jei tyrimas atskleidžia gerą rūgšties slopinimą esant minimaliam rūgšties refliuksui, GERL diagnozė gali būti klaidinga ir reikia ieškoti kitų simptomų priežasčių.
pH tyrimas taip pat gali būti naudojamas siekiant įvertinti, ar refliuksas yra simptomų (dažniausiai rėmens) priežastis. Norėdami atlikti šį įvertinimą, pacientai registruoja kiekvieną kartą, kai jiems pasireiškia simptomai, kol yra atliekamas 24 valandų pH tyrimas. Tada, kai analizuojamas testas, galima nustatyti, ar simptomų metu atsirado rūgšties refliuksas, ar ne. Jei refliuksas pasireiškė tuo pačiu metu kaip ir simptomai, tikėtina, kad refliuksas yra simptomų priežastis. Jei simptomų atsiradimo metu refliukso nebuvo, mažai tikėtina, kad refliuksas bus simptomų priežastis.
Galiausiai, pH tyrimas gali būti naudojamas pacientams įvertinti prieš endoskopinį ar chirurginį GERL gydymą. Kaip aptarta aukščiau, maždaug 20 % pacientų simptomai sumažės, net jei jie neserga GERL (placebo efektas). Prieš atliekant endoskopinį ar chirurginį gydymą, svarbu identifikuoti šiuos pacientus, nes jiems gydymas greičiausiai nebus naudingas. PH tyrimas gali būti naudojamas šiems pacientams identifikuoti, nes jie turės normalų rūgšties refliukso kiekį.
A newer method for prolonged measurement (48 hours) of acid exposure in the esophagus utilizes a small, wireless capsule that is attached to the esophagus just above the LES. The capsule is passed to the lower esophagus by a tube inserted through either the mouth or the nose. After the capsule is attached to the esophagus, the tube is removed. The capsule measures the acid refluxing into the esophagus and transmits this information to a receiver that is worn at the waist. After the study, usually after 48 hours, the information from the receiver is downloaded into a computer and analyzed. The capsule falls off of the esophagus after 3-5 days and is passed in the stool. (The capsule is not reused.)
The advantage of the capsule over standard pH testing is that there is no discomfort from a catheter that passes through the throat and nose. Moreover, with the capsule, patients look normal (they don't have a catheter protruding from their noses) and are more likely to go about their daily activities, for example, go to work, without feeling self-conscious. Because the capsule records for a longer period than the catheter (48 versus 24 hours), more data on acid reflux and symptoms are obtained. Nevertheless, it is not clear whether obtaining additional information is important.
Capsule pH testing is expensive. Sometimes the capsule does not attach to the esophagus or falls off prematurely. For periods of time the receiver may not receive signals from the capsule, and some of the information about reflux of acid may be lost. Occasionally there is pain with swallowing after the capsule has been placed, and the capsule may need to be removed endoscopically. Use of the capsule is an exciting use of new technology although it has its own specific problems.
Esophageal motility testing determines how well the muscles of the esophagus are working. For motility testing, a thin tube (catheter) is passed through a nostril, down the back of the throat, and into the esophagus. On the part of the catheter that is inside the esophagus are sensors that sense pressure. A pressure is generated within the esophagus that is detected by the sensors on the catheter when the muscle of the esophagus contracts. The end of the catheter that protrudes from the nostril is attached to a recorder that records the pressure. During the test, the pressure at rest and the relaxation of the lower esophageal sphincter are evaluated. The patient then swallows sips of water to evaluate the contractions of the esophagus.
Esophageal motility testing has two important uses in evaluating GERD. The first is in evaluating symptoms that do not respond to treatment for GERD since the abnormal function of the esophageal muscle sometimes causes symptoms that resemble the symptoms of GERD. Motility testing can identify some of these abnormalities and lead to a diagnosis of an esophageal motility disorder. The second use is evaluation prior to surgical or endoscopic treatment for GERD. In this situation, the purpose is to identify patients who also have motility disorders of the esophageal muscle. The reason for this is that in patients with motility disorders, some surgeons will modify the type of surgery they perform for GERD.
Gastric emptying studies are studies that determine how well food empties from the stomach. As discussed above, about 20 % of patients with GERD have slow emptying of the stomach that may be contributing to the reflux of acid. For gastric emptying studies, the patient eats a meal that is labeled with a radioactive substance. A sensor that is similar to a Geiger counter is placed over the stomach to measure how quickly the radioactive substance in the meal empties from the stomach.
Information from the emptying study can be useful for managing patients with GERD. For example, if a patient with GERD continues to have symptoms despite treatment with the usual medications, doctors might prescribe other medications that speed-up emptying of the stomach. Alternatively, in conjunction with GERD surgery, they might do a surgical procedure that promotes a more rapid emptying of the stomach. Nevertheless, it is still debated whether a finding of reduced gastric emptying should prompt changes in the surgical treatment of GERD.
Symptoms of nausea, vomiting, and regurgitation may be due either to abnormal gastric emptying or GERD. An evaluation of gastric emptying, therefore, may be useful in identifying patients whose symptoms are due to abnormal emptying of the stomach rather than to GERD.
The acid perfusion (Bernstein) test is used to determine if chest pain is caused by acid reflux. For the acid perfusion test, a thin tube is passed through one nostril, down the back of the throat, and into the middle of the esophagus. A dilute, acid solution and a physiologic salt solution (similar to the fluid that bathes the body's cells) are alternately poured (perfused) through the catheter and into the esophagus. The patient is unaware of which solution is being infused. If the perfusion with acid provokes the patient's usual pain and perfusion of the salt solution produces no pain, it is likely that the patient's pain is caused by acid reflux.
The acid perfusion test, however, is used only rarely. A better test for correlating pain and acid reflux is a 24-hour esophageal pH or pH capsule study during which patients note when they are having pain. It then can be determined from the pH recording if there was an episode of acid reflux at the time of the pain. This is the preferable way of deciding if acid reflux is causing a patient's pain. It does not work well, however, for patients who have infrequent pain, for example every two to three days, which may be missed by a one or two day pH study. In these cases, an acid perfusion test may be reasonable.
One of the simplest treatments for GERD is referred to as life-style changes, a combination of several changes in habit, particularly related to eating.
As discussed above, reflux of acid is more injurious at night than during the day. At night, when individuals are lying down, it is easier for reflux to occur. The reason that it is easier is because gravity is not opposing the reflux, as it does in the upright position during the day. In addition, the lack of an effect of gravity allows the refluxed liquid to travel further up the esophagus and remain in the esophagus longer. These problems can be overcome partially by elevating the upper body in bed. The elevation is accomplished either by putting blocks under the bed's feet at the head of the bed or, more conveniently, by sleeping with the upper body on a foam rubber wedge. These maneuvers raise the esophagus above the stomach and partially restore the effects of gravity. It is important that the upper body and not just the head be elevated. Elevating only the head does not raise the esophagus and fails to restore the effects of gravity.
Elevation of the upper body at night generally is recommended for all patients with GERD. Nevertheless, most patients with GERD have reflux only during the day and elevation at night is of little benefit for them. It is not possible to know for certain which patients will benefit from elevation at night unless acid testing clearly demonstrates night reflux. However, patients who have heartburn, regurgitation, or other symptoms of GERD at night are probably experiencing reflux at night and definitely should elevate their upper body when sleeping. Reflux also occurs less frequently when patients lie on their left rather than their right sides.
Several changes in eating habits can be beneficial in treating GERD. Reflux is worse following meals. This probably is so because the stomach is distended with food at that time and transient relaxations of the lower esophageal sphincter are more frequent. Therefore, smaller and earlier evening meals may reduce the amount of reflux for two reasons. First, the smaller meal results in lesser distention of the stomach. Second, by bedtime, a smaller and earlier meal is more likely to have emptied from the stomach than is a larger one. As a result, reflux is less likely to occur when patients with GERD lie down to sleep.
Certain foods are known to reduce the pressure in the lower esophageal sphincter and thereby promote reflux. These foods should be avoided and include:
Fatty foods (which should be decreased) and smoking (which should be stopped) also reduce the pressure in the sphincter and promote reflux.
In addition, patients with GERD may find that other foods aggravate their symptoms. Examples are spicy or acid-containing foods, like citrus juices, carbonated beverages, and tomato juice. These foods should also be avoided if they provoke symptoms.
One novel approach to the treatment of GERD is chewing gum. Chewing gum stimulates the production of more bicarbonate-containing saliva and increases the rate of swallowing. After the saliva is swallowed, it neutralizes acid in the esophagus. In effect, chewing gum exaggerates one of the normal processes that neutralize acid in the esophagus. It is not clear, however, how effective chewing gum is in treating heartburn. Nevertheless, chewing gum after meals is certainly worth a try.
There is a variety of over-the-counter (for example, antacids and foam barriers) and prescription medications (for example, proton pump inhibitors, histamine antagonists, and promotility drugs) for treating GERD.
Despite the development of potent medications for the treatment of GERD, antacids remain a mainstay of treatment. Antacids neutralize the acid in the stomach so that there is no acid to reflux. The problem with antacids is that their action is brief. They are emptied from the empty stomach quickly, in less than an hour, and the acid then re-accumulates. The best way to take antacids, therefore, is approximately one hour after meals, which is just before the symptoms of reflux begin after a meal. Since the food from meals slows the emptying from the stomach, an antacid taken after a meal stays in the stomach longer and is effective longer. For the same reason, a second dose of antacids approximately two hours after a meal takes advantage of the continuing post-meal slower emptying of the stomach and replenishes the acid-neutralizing capacity within the stomach.
Antacids may be aluminum, magnesium, or calcium-based. Calcium-based antacids (usually calcium carbonate), unlike other antacids, stimulate the release of gastrin from the stomach and duodenum. Gastrin is the hormone that is primarily responsible for the stimulation of acid secretion by the stomach. Therefore, the secretion of acid rebounds after the direct acid-neutralizing effect of the calcium carbonate is exhausted. The rebound is due to the release of gastrin, which results in an overproduction of acid. Theoretically at least, this increased acid is not good for GERD.
Acid rebound, however, is not clinically important. That is, treatment with calcium carbonate is not less effective or safe than treatment with antacids not containing calcium carbonate. Nevertheless, the phenomenon of acid rebound is theoretically harmful. In practice, therefore, calcium-containing antacids such as Tums and Rolaids are not recommended for frequent use. The occasional use of these calcium carbonate-containing antacids, however, is not believed to be harmful. The advantages of calcium carbonate-containing antacids are their low cost, the calcium they add to the diet, and their convenience as compared to liquids.
Aluminum-containing antacids tend to cause constipation, while magnesium-containing antacids tend to cause diarrhea. If diarrhea or constipation becomes a problem, it may be necessary to switch antacids, or use antacids containing both aluminum and magnesium.
Although antacids can neutralize acid, they do so for only a short period. For substantial neutralization of acid throughout the day, antacids would need to be given frequently, at least every hour.
The first medication developed for the more effective and convenient treatment of acid-related diseases, including GERD, was a histamine antagonist, specifically cimetidine (Tagamet). Histamine is an important chemical because it stimulates acid production by the stomach. Released within the wall of the stomach, histamine attaches to receptors (binders) on the stomach's acid-producing cells and stimulates the cells to produce acid. Histamine antagonists work by blocking the receptor for histamine and thereby preventing histamine from stimulating the acid-producing cells. (Histamine antagonists are referred to as H2 antagonists because the specific receptor they block is the histamine type 2 receptor.)
As histamine is particularly important for the stimulation of acid after meals, H2 antagonists are best taken 30 minutes before meals. The reason for this timing is so that the H2 antagonists will be at peak levels in the body after the meal when the stomach is actively producing acid. H2 antagonists also can be taken at bedtime to suppress the nighttime production of acid.
H2 antagonists are very good for relieving the symptoms of GERD, particularly heartburn. However, they are not very good for healing the inflammation (esophagitis) that may accompany GERD. They are used primarily for the treatment of heartburn in GERD that is not associated with inflammation or complications, such as erosions or ulcers, strictures, or Barrett's esophagus.
Three different H2 antagonists are available by prescription, including cimetidine (Tagamet), nizatidine (Axid), and famotidine (Pepcid). Two of these, cimetidine (Tagamet HB) and famotidine (Pepcid AC, Zantac 360) are available over-the-counter (OTC), without the need for a prescription. However, the OTC dosages are lower than those available by prescription.
The second type of drug developed specifically for acid-related diseases, such as GERD, was a proton pump inhibitor (PPI), specifically, omeprazole (Prilosec). A PPI blocks the secretion of acid into the stomach by the acid-secreting cells. The advantage of a PPI over an H2 antagonist is that the PPI shuts off acid production more completely and for a longer period of time. Not only is the PPI good for treating the symptom of heartburn, but it also is good for protecting the esophagus from acid so that esophageal inflammation can heal.
PPIs are used when H2 antagonists do not relieve symptoms adequately or when complications of GERD such as erosions or ulcers, strictures, or Barrett's esophagus exist. Five different PPIs are approved for the treatment of GERD, including omeprazole (Prilosec, Dexilant), lansoprazole (Prevacid), rabeprazole (Aciphex), pantoprazole (Protonix), and esomeprazole (Nexium), and dexlansoprazole (Dexilant). A sixth PPI product consists of a combination of omeprazole and sodium bicarbonate (Zegerid). PPIs (except for Zegerid) are best taken an hour before meals. The reason for this timing is that the PPIs work best when the stomach is most actively producing acid, which occurs after meals. If the PPI is taken before the meal, it is at peak levels in the body after the meal when the acid is being made.
Pro-motility drugs work by stimulating the muscles of the gastrointestinal tract, including the esophagus, stomach, small intestine, and/or colon. One pro-motility drug, metoclopramide (Reglan), is approved for GERD. Pro-motility drugs increase the pressure in the lower esophageal sphincter and strengthen the contractions (peristalsis) of the esophagus. Both effects would be expected to reduce the reflux of acid. However, these effects on the sphincter and esophagus are small. Therefore, it is believed that the primary effect of metoclopramide may be to speed up emptying of the stomach, which also would be expected to reduce reflux.
Pro-motility drugs are most effective when taken 30 minutes before meals and again at bedtime. They are not very effective for treating either the symptoms or complications of GERD. Therefore, the pro-motility agents are reserved either for patients who do not respond to other treatments or are added to enhance other treatments for GERD.
Foam barriers provide a unique form of treatment for GERD. Foam barriers are tablets that are composed of an antacid and a foaming agent. As the tablet disintegrates and reaches the stomach, it turns into foam that floats on top of the liquid contents of the stomach. The foam forms a physical barrier to the reflux of liquid. At the same time, the antacid bound to the foam neutralizes acid that comes into contact with the foam. The tablets are best taken after meals (when the stomach is distended) and when lying down, both times when reflux is more likely to occur. Foam barriers are not often used as the first or only treatment for GERD. Rather, they are added to other drugs for GERD when the other drugs are not adequately effective in relieving symptoms. There is only one foam barrier, which is a combination of aluminum hydroxide gel, magnesium trisilicate, and alginate (Gaviscon).
The drugs described above usually are effective in treating the symptoms and complications of GERD. Nevertheless, sometimes they are not. For example, despite adequate suppression of acid and relief from heartburn, regurgitation, with its potential for complications in the lungs, may still occur. Moreover, the amounts and/or numbers of drugs that are required for satisfactory treatment are sometimes so great that drug treatment is unreasonable. In such situations, surgery can effectively stop reflux.
The surgical procedure that is done to prevent reflux is technically known as fundoplication and is called reflux surgery or anti-reflux surgery. During fundoplication, any hiatal hernial sac is pulled below the diaphragm and stitched there. In addition, the opening in the diaphragm through which the esophagus passes is tightened around the esophagus. Finally, the upper part of the stomach next to the opening of the esophagus into the stomach is wrapped around the lower esophagus to make an artificial lower esophageal sphincter. All of this surgery can be done through an incision in the abdomen (laparotomy) or using a technique called laparoscopy. During laparoscopy, a small viewing device and surgical instruments are passed through several small puncture sites in the abdomen. This procedure avoids the need for a major abdominal incision.
Surgery is very effective at relieving symptoms and treating the complications of GERD. Approximately 80% of patients will have good or excellent relief of their symptoms for at least 5 to 10 years. Nevertheless, many patients who have had surgery will continue to take drugs for reflux. It is not clear whether they take the drugs because they continue to have reflux and symptoms of reflux or if they take them for symptoms that are being caused by problems other than GERD. The most common complication of fundoplication is swallowed food that sticks at the artificial sphincter. Fortunately, the sticking usually is temporary. If it is not transient, endoscopic treatment to stretch (dilate) the artificial sphincter usually will relieve the problem. Only occasionally is it necessary to re-operate to revise the prior surgery.
Very recently, endoscopic techniques for the treatment of GERD have been developed and tested. One type of endoscopic treatment involves suturing (stitching) the area of the lower esophageal sphincter, which essentially tightens the sphincter.
A second type involves the application of radio-frequency waves to the lower part of the esophagus just above the sphincter. The waves cause damage to the tissue beneath the esophageal lining and a scar (fibrosis) forms. The scar shrinks and pulls on the surrounding tissue, thereby tightening the sphincter and the area above it.
A third type of endoscopic treatment involves the injection of materials into the esophageal wall in the area of the LES. The injected material is intended to increase pressure in the LES and thereby prevent reflux. In one treatment the injected material was a polymer. Unfortunately, the injection of polymer led to serious complications, and the material for injection is no longer available. Another treatment involving injection of expandable pellets also was discontinued. Limited information is available about a third type of injection which uses gelatinous polymethylmethacrylate microspheres.
Endoscopic treatment has the advantage of not requiring surgery. It can be performed without hospitalization. Experience with endoscopic techniques is limited. It is not clear how effective they are, especially long-term. Because the effectiveness and the full extent of potential complications of endoscopic techniques are not clear, it is felt generally that endoscopic treatment should only be done as part of experimental trials.
Transient LES relaxations appear to be the most common way in which acid reflux occurs. Although there is an available drug that prevents relaxations (baclofen), it has side effects that are too frequent to be generally useful. Much attention is being directed at the development of drugs that prevent these relaxations without accompanying side effects.
There are several ways to approach the evaluation and management of GERD. The approach depends primarily on the frequency and severity of symptoms, the adequacy of the response to treatment, and the presence of complications.
For infrequent heartburn, the most common symptom of GERD, life-style changes and an occasional antacid may be all that is necessary. If heartburn is frequent, daily non-prescription-strength (over-the-counter) H2 antagonists may be adequate. A foam barrier also can be used with the antacid or H2 antagonist.
If life-style changes and antacids, non-prescription H2 antagonists, and a foam barrier do not adequately relieve heartburn, it is time to see a physician for further evaluation and to consider prescription-strength drugs. The evaluation by the physician should include an assessment for possible complications of GERD based on the presence of such symptoms or findings as:
Clues to the presence of diseases that may mimic GERD, such as gastric or duodenal ulcers and esophageal motility disorders, should be sought.
If there are no symptoms or signs of complications and no suspicion of other diseases, a therapeutic trial of acid suppression with H2 antagonists often is used. If H2 antagonists are not adequately effective, a second trial, with the more potent PPIs, can be given. Sometimes, a trial of treatment begins with a PPI and skips the H2 antagonist. If treatment relieves the symptoms completely, no further evaluation may be necessary and the effective drug, the H2 antagonist or PPI, is continued. As discussed previously, however, there are potential problems with this commonly used approach, and some physicians would recommend a further evaluation for almost all patients they see.
If at the time of evaluation, there are symptoms or signs that suggest complicated GERD or a disease other than GERD or if the relief of symptoms with H2 antagonists or PPIs is not satisfactory, a further evaluation by endoscopy (EGD) definitely should be done.
There are several possible results of endoscopy and each requires a different approach to treatment. If the esophagus is normal and no other diseases are found, the goal of treatment simply is to relieve symptoms. Therefore, prescription strength H2 antagonists or PPIs are appropriate. If damage to the esophagus (esophagitis or ulceration) is found, the goal of treatment is healing the damage. In this case, PPIs are preferred over H2 antagonists because they are more effective for healing.
If complications of GERD, such as stricture or Barrett's esophagus are found, treatment with PPIs also is more appropriate. However, the adequacy of the PPI treatment probably should be evaluated with a 24-hour pH study during treatment with the PPI. (With PPIs, although the amount of acid reflux may be reduced enough to control symptoms, it may still be abnormally high. Therefore, judging the adequacy of suppression of acid reflux by only the response of symptoms to treatment is not satisfactory.) Strictures may also need to be treated by endoscopic dilatation (widening) of the esophageal narrowing. With Barrett's esophagus, periodic endoscopic examination should be done to identify pre-malignant changes in the esophagus.
If symptoms of GERD do not respond to maximum doses of PPI, there are two options for management. The first is to perform 24-hour pH testing to determine whether the PPI is ineffective or if a disease other than GERD is likely to be present. If the PPI is ineffective, a higher dose of PPI may be tried. The second option is to go ahead without 24 hour pH testing and to increase the dose of PPI. Another alternative is to add another drug to the PPI that works in a way that is different from the PPI, for example, a pro-motility drug or a foam barrier. If necessary, all three types of drugs can be used. If there is not a satisfactory response to this maximal treatment, 24 hour pH testing should be done.
Who should consider surgery or, perhaps, an endoscopic treatment trial for GERD? (As mentioned previously, the effectiveness of the recently developed endoscopic treatments remains to be determined.) Patients should consider surgery if they have regurgitation that cannot be controlled with drugs. This recommendation is particularly important if the regurgitation results in infections in the lungs or occurs at night when aspiration into the lungs is more likely. Patients also should consider surgery if they require large doses of PPI or multiple drugs to control their reflux. It is debated whether or not a desire to be free of the need to take life-long drugs to prevent symptoms of GERD is by itself a satisfactory reason for having surgery.
Some physicians - primarily surgeons - recommend that all patients with Barrett's esophagus should have surgery. This recommendation is based on the belief that surgery is more effective than endoscopic surveillance or ablation of the abnormal tissue followed by treatment with acid-suppressing drugs in preventing both the reflux and the cancerous changes in the esophagus. There are no studies, however, demonstrating the superiority of surgery over drugs or ablation for the treatment of GERD and its complications. Moreover, the effectiveness of drug treatment can be monitored with 24 hour pH testing.
One unresolved issue in GERD is the inconsistent relationships among acid reflux, heartburn, and damage to the lining of the esophagus (esophagitis and the complications).
Clearly, we have much to learn about the relationship between acid reflux and esophageal damage, and about the processes (mechanisms) responsible for heartburn. This issue is of more than passing interest. Knowledge of the mechanisms that produce heartburn and esophageal damage raises the possibility of new treatments that would target processes other than acid reflux.
One of the more interesting theories that has been proposed to answer some of these questions involves the reason for pain when acid refluxes. It often is assumed that the pain is caused by irritating acid contacting an inflamed esophageal lining. But the esophageal lining usually is not inflamed. It is possible therefore, that the acid is stimulating the pain nerves within the esophageal wall just beneath the lining. Although this may be the case, a second explanation is supported by the work of one group of scientists. These scientists find that heartburn provoked by acid in the esophagus is associated with contraction of the muscle in the lower esophagus. Perhaps it is the contraction of the muscle that somehow leads to the pain. It also is possible, however, that the contraction is an epiphenomenon, that is, refluxed acid stimulates pain nerves and causes the muscle to contract, but it is not the contraction that causes the pain. More studies will be necessary before the exact mechanism(s) that causes heartburn is clear.
There are potentially injurious agents that can be refluxed other than acid, for example, bile. Until recently it has been impossible or difficult to accurately identify non-acid reflux and, therefore, to study whether or not non-acid reflux is injurious or can cause symptoms.
A new technology allows the accurate determination of non-acid reflux. This technology uses the measurement of impedance changes within the esophagus to identify reflux of liquid, be it acid or non-acid. By combining measurement of impedance and pH it is possible to identify reflux and to tell if the reflux is acid or non-acid. It is too early to know how important non-acid reflux is in causing esophageal damage, symptoms, or complications, but there is little doubt that this new technology will be able to resolve the issues surrounding non-acid reflux.
 JFK sirgo celiakija ir kolitu?
JFK sirgo celiakija ir kolitu?
 IBD ir Krono ligos pašalinimo dieta (enteralinė mityba)
IBD ir Krono ligos pašalinimo dieta (enteralinė mityba)
 Hiperkalcemija (padidėjęs kalcio kiekis)
Hiperkalcemija (padidėjęs kalcio kiekis)
 Ar Parkinsono liga gali prasidėti žarnyne?
Ar Parkinsono liga gali prasidėti žarnyne?
 Bacon Pemmican – geriausias paleo kelionių maistas
Bacon Pemmican – geriausias paleo kelionių maistas
 Padidėjusios blužnies (splenomegalija) simptomai, požymiai, priežastys ir gydymas
Padidėjusios blužnies (splenomegalija) simptomai, požymiai, priežastys ir gydymas
 Gerklų vėžio apžvalga
Gerklų vėžys yra vėžio rūšis, pažeidžianti gerklas – organą, kurį paprastai žinome kaip balso dėžutę. Maždaug 12 500 amerikiečių kasmet diagnozuojamas gerklų vėžys, iš kurių maždaug 3 500 mirs nuo šio
Gerklų vėžio apžvalga
Gerklų vėžys yra vėžio rūšis, pažeidžianti gerklas – organą, kurį paprastai žinome kaip balso dėžutę. Maždaug 12 500 amerikiečių kasmet diagnozuojamas gerklų vėžys, iš kurių maždaug 3 500 mirs nuo šio
 Kas sukelia vėmimą? 7 priežastys, kodėl ir kaip tai palengvinti
Kokios yra septynios dažniausiai pasitaikančios vėmimo priežastys? Rytinis pykinimas nėštumo metu – dažna vėmimo priežastis. Vėmimas yra refleksas, kurį smegenys nukreipia į žarnyną, kad pakeistų
Kas sukelia vėmimą? 7 priežastys, kodėl ir kaip tai palengvinti
Kokios yra septynios dažniausiai pasitaikančios vėmimo priežastys? Rytinis pykinimas nėštumo metu – dažna vėmimo priežastis. Vėmimas yra refleksas, kurį smegenys nukreipia į žarnyną, kad pakeistų
 Žarnyno mikrobiomas gali turėti įtakos sunkiam COVID-19
Dabartinę pasaulinę COVID-19 pandemiją sukelia sunkus beta koronaviruso ūminis kvėpavimo sindromas koronavirusas-2 (SARS-CoV-2), visame pasaulyje užkrėtė daugiau nei 22,1 mln. ir mirė 780 tūkst. Viena
Žarnyno mikrobiomas gali turėti įtakos sunkiam COVID-19
Dabartinę pasaulinę COVID-19 pandemiją sukelia sunkus beta koronaviruso ūminis kvėpavimo sindromas koronavirusas-2 (SARS-CoV-2), visame pasaulyje užkrėtė daugiau nei 22,1 mln. ir mirė 780 tūkst. Viena