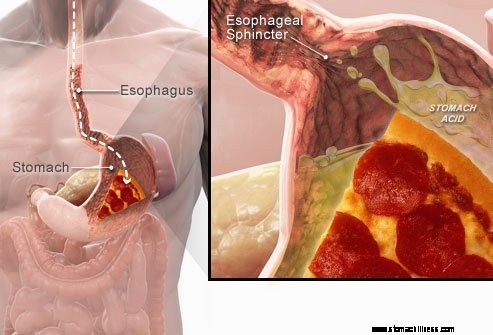
 När du sväljer mat åker den ner i matstrupen och passerar genom en muskelring som kallas den nedre esofagusfinktern ( LES). Denna struktur öppnar för att tillåta mat att passera in i magen. Den ska förbli stängd för att hålla maginnehållet där det hör hemma.
När du sväljer mat åker den ner i matstrupen och passerar genom en muskelring som kallas den nedre esofagusfinktern ( LES). Denna struktur öppnar för att tillåta mat att passera in i magen. Den ska förbli stängd för att hålla maginnehållet där det hör hemma.
Symtom på GERD eller sura uppstötningar orsakas av uppstötningar av surt flytande maginnehåll tillbaka upp i matstrupen. Det vanligaste symtomet på GERD är halsbränna.
Andra symtom som kan uppstå som ett resultat av GERD inkluderar:
 Det vanligaste symtomet på GERD är halsbränna.
Det vanligaste symtomet på GERD är halsbränna. Gastroesofageal refluxsjukdom, vanligen kallad GERD eller sura uppstötningar, är ett tillstånd där vätskeinnehållet i magsäcken regurgitates (back-up eller refluxes) in i matstrupen. Vätskan kan inflammera och skada slemhinnan (esofagit) även om synliga tecken på inflammation förekommer hos en minoritet av patienterna. Den uppstötade vätskan innehåller vanligtvis syra och pepsin som produceras av magen. (Pepsin är ett enzym som startar nedbrytningen av proteiner i magen.) Den återloppskokta vätskan kan också innehålla galla som har kommit in i magen från tolvfingertarmen. Den första delen av tunntarmen fäst vid magen. Syra tros vara den mest skadliga komponenten i den återloppskokta vätskan. Pepsin och galla kan också skada matstrupen, men deras roll i produktionen av matstrupsinflammation och skador är inte lika tydlig som syrans roll.
GERD är ett kroniskt tillstånd. När det väl börjar är det vanligtvis livslångt. Om det finns en skada på slemhinnan i matstrupen (esofagit) är detta också ett kroniskt tillstånd. Dessutom, efter att matstrupen har läkt med behandling och behandlingen avbryts, kommer skadan tillbaka hos de flesta patienter inom några månader. När behandlingen för GERD väl har påbörjats kommer den att behöva fortsätta på obestämd tid. Vissa patienter med intermittenta symtom och ingen esofagit kan dock endast behandlas under symtomatiska perioder.
Faktum är att reflux av magens flytande innehåll i matstrupen förekommer hos de flesta normala individer. En studie fann att reflux förekommer ofta hos normala individer som hos patienter med GERD. Hos patienter med GERD innehåller återflödesvätskan dock oftare syra, och syran stannar kvar i matstrupen längre. Det har också visat sig att flytande refluxer till en högre nivå i matstrupen hos patienter med GERD än hos normala individer.
Som ofta är fallet har kroppen sätt att skydda sig mot de skadliga effekterna av reflux och syra. Till exempel inträffar de flesta reflux under dagen när individer är upprätt. I upprätt läge är det mer sannolikt att den återloppskokade vätskan rinner tillbaka ner i magen på grund av gravitationens inverkan. Dessutom, medan individer är vakna, sväljer de upprepade gånger, oavsett om det finns reflux eller inte. Varje svälja bär eventuell återflödesvätska tillbaka in i magen. Slutligen producerar spottkörtlarna i munnen saliv, som innehåller bikarbonat. Med varje svälj vandrar bikarbonatinnehållande saliv ner i matstrupen. Bikarbonatet neutraliserar den lilla mängd syra som finns kvar i matstrupen efter att gravitationen och sväljningen har avlägsnat det mesta av den sura vätskan.
Gravitation, sväljning och saliv är viktiga skyddsmekanismer för matstrupen, men de är effektiva endast när individer är i upprätt position. På natten under sömnen har gravitationen ingen effekt, sväljningen upphör och salivutsöndringen minskar. Därför är det mer sannolikt att reflux som inträffar på natten resulterar i att syra stannar kvar i matstrupen längre och orsakar större skada på matstrupen.
Vissa tillstånd gör en person mottaglig för GERD. Till exempel kan GERD vara ett allvarligt problem under graviditeten. De förhöjda hormonnivåerna under graviditeten orsakar troligen reflux genom att sänka trycket i den nedre esofagusfinktern (se nedan). Samtidigt ökar det växande fostret trycket i buken. Båda dessa effekter skulle förväntas öka reflux. Dessutom är patienter med sjukdomar som försvagar matstrupsmusklerna, såsom sklerodermi eller blandade bindvävssjukdomar, mer benägna att utveckla GERD.
Orsaken till GERD är komplex och kan involvera flera orsaker. Dessutom kan olika orsaker påverka olika individer eller till och med hos samma individ vid olika tidpunkter. Ett litet antal patienter med GERD producerar onormalt stora mängder syra, men detta är ovanligt och inte en bidragande faktor hos de allra flesta patienter.
Faktorerna som bidrar till GERD är:
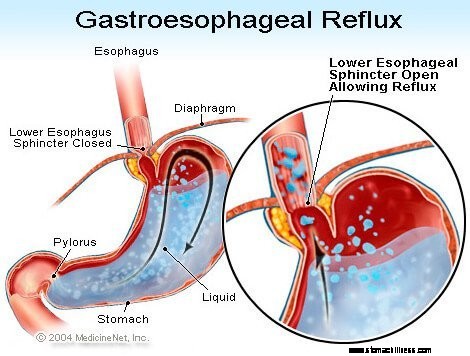
Verkan av den nedre esofagusfinktern (LES) är kanske den viktigaste faktorn (mekanismen) för att förhindra reflux. Matstrupen är ett muskulärt rör som sträcker sig från nedre halsen till magsäcken. LES är en specialiserad muskelring som omger den nedre änden av matstrupen där den förenas med magen. Muskeln som utgör LES är aktiv för det mesta, det vill säga i vila. Detta innebär att det drar ihop sig och stänger av passagen från matstrupen in i magsäcken. Denna stängning av passagen förhindrar återflöde. När mat eller saliv sväljs slappnar LES av i några sekunder så att maten eller saliven kan passera från matstrupen in i magsäcken och sedan stänger den igen.
Flera olika abnormiteter av LES har hittats hos patienter med GERD. Två av dem involverar LES-funktionen. Den första är onormalt svag sammandragning av LES, vilket minskar dess förmåga att förhindra reflux. Den andra är onormala avslappningar av LES, som kallas övergående LES-avslappningar. De är onormala genom att de inte följer med svalor och de håller länge, upp till flera minuter. Dessa långvariga avslappningar gör att reflux uppstår lättare. De övergående LES-avslappningarna inträffar hos patienter med GERD oftast efter måltider när magen är utspänd av mat. Övergående LES-avslappningar förekommer också hos individer utan GERD, men de är sällsynta.
Den senast beskrivna abnormiteten hos patienter med GERD är slappheten i LES. Specifikt, liknande utvidgningstryck öppnar LES mer hos patienter med GERD än hos individer utan GERD. Åtminstone teoretiskt skulle detta möjliggöra enklare öppning av LES och/eller större bakåtflöde av syra in i matstrupen när LES är öppen.
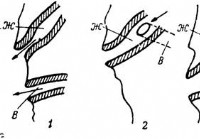
Hiatalbråck bidrar till reflux, även om det inte är klart på vilket sätt de bidrar. En majoritet av patienter med GERD har hiatalbråck, men många har inte. Därför är det inte nödvändigt att ha ett hiatalbråck för att få GERD. Dessutom har många människor hiatalbråck men har inte GERD. Det är inte säkert känt hur eller varför hiatalbråck utvecklas.
Normalt ligger LES på samma nivå där matstrupen passerar från bröstet genom en liten öppning i mellangärdet och in i buken. (Diafragman är en muskulös, horisontell skiljevägg som skiljer bröstet från buken.) När det finns ett hiatalbråck trycker en liten del av den övre magsäcken som fäster vid matstrupen upp genom diafragman. Som ett resultat kommer en liten del av magen och LES att ligga i bröstet, och LES är inte längre i nivå med diafragman.
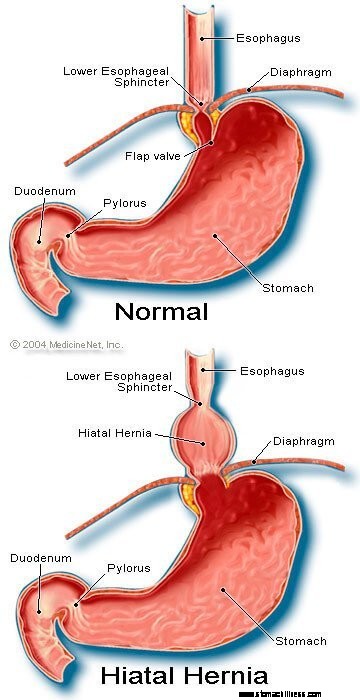 Bild på Hiatal bråck
Bild på Hiatal bråck
Det verkar som om diafragman som omger LES är viktig för att förhindra reflux. Det vill säga, hos individer utan hiatalbråck dras diafragman som omger matstrupen kontinuerligt ihop, men slappnar sedan av med sväljning, precis som LES. Observera att effekterna av LES och diafragman uppträder på samma plats hos patienter utan hiatalbråck. Därför är barriären mot återflöde lika med summan av trycken som genereras av LES och diafragman. När LES rör sig in i bröstet med ett hiatal bråck, fortsätter diafragman och LES att utöva sina tryck och barriäreffekt. Men nu gör de det på olika platser. Följaktligen är trycken inte längre additiv. Istället ersätts en enda högtrycksbarriär mot återflöde med två barriärer med lägre tryck, och återflöde uppstår därmed lättare. Så att minska tryckbarriären är ett sätt som ett hiatalbråck kan bidra till reflux.
Som tidigare nämnt är svalor viktiga för att eliminera syra i matstrupen. Sväljning orsakar en ringliknande våg av sammandragning av matstrupsmusklerna, vilket minskar lumen (inre hålighet) i matstrupen. Sammandragningen, som kallas peristaltiken, börjar i övre matstrupen och går till nedre matstrupen. Det trycker in mat, saliv och allt annat som finns i matstrupen i magen.
När sammandragningsvågen är defekt, trycks inte refluxsyra tillbaka in i magen. Hos patienter med GERD har flera abnormiteter av kontraktion beskrivits. Till exempel kanske sammandragningsvågor inte börjar efter varje svälj eller så kan sammandragningsvågorna dö ut innan de når magen. Dessutom kan trycket som genereras av sammandragningarna vara för svagt för att trycka tillbaka syran i magen. Sådana abnormiteter av kontraktion, som minskar clearance av syra från matstrupen, finns ofta hos patienter med GERD. I själva verket finns de oftast hos de patienter med den svåraste GERD. Effekterna av onormala esofagussammandragningar skulle förväntas bli värre på natten när gravitationen inte hjälper till att återföra återflödessyra till magsäcken. Observera att rökning också avsevärt minskar clearance av syra från matstrupen. Denna effekt fortsätter i minst 6 timmar efter den sista cigaretten.
Mest reflux under dagen sker efter måltider. Denna reflux beror troligen på övergående LES-avslappningar som orsakas av utvidgning av magen med mat. En minoritet av patienter med GERD, ungefär, har visat sig ha magar som töms onormalt långsamt efter en måltid. Detta kallas gastropares. Den långsammare tömningen av magsäcken förlänger magsäckens utvidgning med mat efter måltider. Därför förlänger den långsammare tömningen den tidsperiod under vilken det är mer sannolikt att återflöde uppstår. Det finns flera mediciner förknippade med nedsatt magtömning, såsom:
Individer bör inte sluta ta dessa eller andra läkemedel som är ordinerade förrän den förskrivande läkaren har diskuterat den potentiella GERD-situationen med dem.
Symtomen på okomplicerad GERD är främst:
Andra symtom uppstår när det finns komplikationer av GERD och kommer att diskuteras med komplikationerna.
När sura uppstötningar återgår till matstrupen hos patienter med GERD, stimuleras nervfibrer i matstrupen. Denna nervstimulering resulterar oftast i halsbränna, den smärta som är karakteristisk för GERD. Halsbränna beskrivs vanligtvis som en brännande smärta i mitten av bröstet. Det kan börja högt upp i buken eller kan sträcka sig upp i nacken. Hos vissa patienter kan dock smärtan vara skarp eller tryckliknande snarare än brännande. Sådan smärta kan härma hjärtsmärta (kärlkramp). Hos andra patienter kan smärtan sträcka sig till ryggen.
Eftersom sura uppstötningar är vanligare efter måltider är halsbränna vanligare efter måltider. Halsbränna är också vanligare när individer ligger ner eftersom utan gravitationens effekter uppstår reflux lättare och syra återförs till magen långsammare. Många patienter med GERD väcks ur sömnen av halsbränna.
Episoder av halsbränna tenderar att inträffa med jämna mellanrum. Detta innebär att episoderna är mer frekventa eller allvarliga under en period av flera veckor eller månader, och sedan blir mindre frekventa eller svåra eller till och med frånvarande under flera veckor eller månader. Denna periodicitet av symtom ger anledningen till intermittent behandling hos patienter med GERD som inte har esofagit. Ändå är halsbränna ett livslångt problem, och det återkommer nästan alltid.
Regurgitation är uppkomsten av återflödesvätska i munnen. Hos de flesta patienter med GERD når vanligtvis endast små mängder vätska till matstrupen och vätskan stannar kvar i den nedre matstrupen. Ibland, hos vissa patienter med GERD, återflödas större mängder vätska, ibland innehållande mat, och når den övre matstrupen.
I den övre änden av matstrupen finns den övre matstrupssfinktern (UES). UES är en cirkulär muskelring som i sina handlingar är mycket lik LES. Det vill säga, UES förhindrar matstrupsinnehållet från att backa upp i halsen. När små mängder återflödesvätska och/eller mat kommer förbi UES och kommer in i halsen kan det finnas en sur smak i munnen. Om större mängder bryter mot UES kan patienter plötsligt hitta munnen fylld med vätskan eller maten. Dessutom kan frekventa eller långvariga uppstötningar leda till syrainducerade erosioner av tänderna.
Illamående är ovanligt vid GERD. Hos vissa patienter kan det dock vara frekvent eller allvarligt och kan leda till kräkningar. Faktum är att hos patienter med oförklarat illamående och/eller kräkningar, är GERD ett av de första tillstånden att överväga. Det är inte klart varför vissa patienter med GERD huvudsakligen utvecklar halsbränna och andra utvecklar huvudsakligen illamående.
Vätskan från magsäcken som återflödet in i matstrupen skadar cellerna som kantar matstrupen. Kroppen reagerar på det sätt som den vanligtvis svarar på skador, vilket är med inflammation (esofagit). Syftet med inflammation är att neutralisera det skadliga medlet och påbörja läkningsprocessen. Om skadan går djupt ner i matstrupen bildas ett sår. Ett sår är helt enkelt ett brott i slemhinnan i matstrupen som uppstår i ett område med inflammation. Sår och den ytterligare inflammation de framkallar kan erodera in i esofagusblodkärlen och ge upphov till blödning i matstrupen.
Ibland är blödningen svår och kan kräva:
Sår i matstrupen läker med bildandet av ärr (fibros). Med tiden krymper ärrvävnaden och smalnar av lumen (inre hålighet) i matstrupen. Denna ärrade förträngning kallas en striktur. Mat som svalts kan fastna i matstrupen när förträngningen blir tillräckligt allvarlig (vanligtvis när den begränsar matstrupens lumen till en diameter på en centimeter). Denna situation kan kräva endoskopisk borttagning av det fastnade maten. Sedan, för att förhindra att maten fastnar, måste förträngningen sträckas ut (vidgas). Dessutom, för att förhindra att förträngningen återkommer, måste reflux också förhindras.
Långvarig och/eller svår GERD orsakar förändringar i cellerna som kantar matstrupen hos vissa patienter. Dessa celler är pre-cancerösa och kan, men vanligtvis, bli cancerösa. Detta tillstånd kallas Barretts matstrupe och förekommer hos cirka 10 % av patienterna med GERD. Typen av matstrupscancer associerad med Barretts matstrupe (adenokarcinom) ökar i frekvens. Det är inte klart varför vissa patienter med GERD utvecklar Barretts esofagus, men de flesta gör det inte.
Barretts matstrupe kan kännas igen visuellt vid tidpunkten för en endoskopi och bekräftas genom mikroskopisk undersökning av slemhinnan. Sedan kan patienter med Barretts matstrupe genomgå periodiska övervakningsendoskopier med biopsier även om det inte råder enighet om vilka patienter som behöver övervakning. Syftet med övervakningen är att upptäcka progression från pre-cancer till mer cancerförändringar så att cancerförebyggande behandling kan påbörjas. Man tror också att patienter med Barretts matstrupe bör få maximal behandling för GERD för att förhindra ytterligare skador på matstrupen. Procedurer studeras för att ta bort de onormala slemhinnorna. Flera endoskopiska, icke-kirurgiska tekniker kan användas för att ta bort cellerna. Dessa tekniker är attraktiva eftersom de inte kräver operation; Det finns dock associerade med komplikationer och den långsiktiga effektiviteten av behandlingarna har ännu inte fastställts. Kirurgiskt avlägsnande av matstrupen är alltid ett alternativ.
Många nerver finns i nedre matstrupen. Vissa av dessa nerver stimuleras av den refluxade syran, och denna stimulering resulterar i smärta (vanligtvis halsbränna). Andra nerver som stimuleras ger inte smärta. Istället stimulerar de ytterligare nerver som framkallar hosta. På så sätt kan återflödesvätska orsaka hosta utan att någonsin nå halsen! På liknande sätt kan reflux i nedre matstrupen stimulera matstrupsnerver som ansluter till och kan stimulera nerver som går till lungorna. Dessa nerver till lungorna kan då göra att de mindre andningsrören blir smalare, vilket resulterar i ett astmaanfall.
Även om GERD kan orsaka hosta, är det inte en vanlig orsak till oförklarlig hosta. Även om GERD också kan vara en orsak till astma, är det mer troligt att det utlöser astmatiska attacker hos patienter som redan har astma. Även om kronisk hosta och astma är vanliga åkommor, är det inte klart hur ofta de förvärras eller orsakas av GERD.
Om refluxad vätska kommer förbi den övre esofagusfinktern kan den komma in i halsen (svalget) och till och med röstlådan (struphuvudet). Den resulterande inflammationen kan leda till halsont och heshet. Precis som med hosta och astma är det inte klart hur ofta GERD är ansvarig för annars oförklarlig inflammation i halsen och struphuvudet.
Återflödesvätska som passerar från svalget (svalget) och in i struphuvudet kan komma in i lungorna (aspiration). Återflödet av vätska i lungorna (kallas aspiration) resulterar ofta i hosta och kvävning. Aspiration kan dock också förekomma utan att dessa symtom uppstår. Med eller utan dessa symtom kan aspiration leda till infektion i lungorna och resultera i lunginflammation. Denna typ av lunginflammation är ett allvarligt problem som kräver omedelbar behandling. När aspiration inte åtföljs av symtom kan det resultera i en långsam, progressiv ärrbildning i lungorna (lungfibros) som kan ses på lungröntgen. Aspiration är mer sannolikt att inträffa på natten eftersom det är när processerna (mekanismerna) som skyddar mot reflux inte är aktiva och hostreflexen som skyddar lungorna inte heller är aktiv.
Halsen kommunicerar med näsgångarna. Hos små barn finns två fläckar av lymfvävnad, som kallas adenoider, där den övre delen av halsen förenar sig med näsgångarna. Passagerna från bihålorna och rören från mellanörat (Eustachian tubes) mynnar ut i baksidan av näsgångarna nära adenoiderna. Återflödesvätska som kommer in i den övre halsen kan inflammera adenoiderna och få dem att svälla. De svullna adenoiderna kan då blockera passagerna från bihålorna och Eustachian-rören. När bihålor och mellanörat stängs av från näsgångarna genom svullnad av adenoiderna, ansamlas vätska i dem. Denna ansamling av vätska kan leda till obehag i bihålor och öron. Eftersom adenoiderna är framträdande hos små barn, och inte hos vuxna, ses denna vätskeansamling i öronen och bihålorna hos barn och inte hos vuxna.
Det finns en mängd olika procedurer, tester och utvärdering av symtom (till exempel halsbränna) för att diagnostisera och utvärdera patienter med GERD.
Det vanliga sättet att GERD är genom dess karakteristiska symptom, halsbränna. Halsbränna beskrivs oftast som en substernal (under mitten av bröstet) sveda som uppstår efter måltider och som ofta förvärras när man ligger ner. För att bekräfta diagnosen behandlar läkare ofta patienter med mediciner för att undertrycka produktionen av syra i magen. Om halsbrännan då minskar i stor utsträckning anses diagnosen GERD vara bekräftad. Detta tillvägagångssätt att ställa en diagnos på grundval av ett svar av symptomen på behandling kallas vanligtvis en terapeutisk prövning.
Det finns problem med detta tillvägagångssätt. Till exempel kan patienter som har tillstånd som kan efterlikna GERD, särskilt duodenalsår eller magsår, faktiskt också svara på sådan behandling. I denna situation, om läkaren antar att problemet är GERD, skulle orsaken till sårsjukdomen missas, såsom en typ av infektion som kallas Helicobacter pylori (H. pylori ), eller icke-steroida antiinflammatoriska läkemedel eller NSAID (till exempel ibuprofen), kan också orsaka sår och dessa tillstånd skulle behandlas annorlunda än GERD.
Dessutom, som med all behandling, finns det kanske en placeboeffekt på 20 %, vilket betyder att 20 % av patienterna kommer att svara på ett placebo-piller (inaktivt) eller, faktiskt, på vilken behandling som helst. Detta innebär att 20 % av patienterna som har andra orsaker till sina symtom än GERD (eller sår) kommer att få en minskning av sina symtom efter att ha fått behandlingen för GERD. På grundval av deras svar på behandlingen (den terapeutiska prövningen), kommer dessa patienter att fortsätta att behandlas för GERD, även om de inte har GERD. Dessutom kommer den verkliga orsaken till deras symtom inte att eftersträvas.
Endoskopi av övre mag-tarmkanalen (även känd som esophago-gastro-duodenoskopi eller EGD) är ett vanligt sätt att diagnostisera GERD. EGD är en procedur där ett rör som innehåller ett optiskt system för visualisering sväljs. När röret fortskrider ner i mag-tarmkanalen kan slemhinnan i matstrupen, magen och tolvfingertarmen undersökas.
Matstrupen hos de flesta patienter med symtom på reflux ser normal ut. Därför hjälper endoskopi hos de flesta patienter inte vid diagnosen GERD. Men ibland verkar slemhinnan i matstrupen inflammerad (esofagit). Dessutom, om erosioner (ytliga brott i esofagusslemhinnan) eller sår (djupare brott i slemhinnan) ses, kan en diagnos av GERD ställas med säkerhet. Endoskopi kommer också att identifiera flera av komplikationerna av GERD, särskilt sår, strikturer och Barretts matstrupe. Biopsier kan också erhållas.
Slutligen kan andra vanliga problem som kan orsaka GERD-liknande symtom diagnostiseras (till exempel sår, inflammation eller cancer i magen eller tolvfingertarmen) med EGD.
Biopsier av matstrupen som erhålls genom endoskopet anses inte vara särskilt användbara för att diagnostisera GERD. De är emellertid användbara för att diagnostisera cancer eller andra orsaker till esofagusinflammation än sura uppstötningar, särskilt infektioner. Dessutom är biopsier det enda sättet att diagnostisera cellförändringarna i Barretts matstrupe. På senare tid har det föreslagits att även hos patienter med GERD vars matstrupe verkar normal för ögat, kommer biopsier att visa vidgning av utrymmena mellan slemhinnecellerna, möjligen en indikation på skada. Det är dock för tidigt att dra slutsatsen att det är tillräckligt specifikt att se utvidgningen för att vara säker på att GERD är närvarande.
Före införandet av endoskopi var en röntgen av matstrupen (kallad esofagram) det enda sättet att diagnostisera GERD. Patienterna svalde barium (kontrastmaterial), och sedan togs röntgenbilder av den bariumfyllda matstrupen. Problemet med esofagrammet var att det var ett okänsligt test för att diagnostisera GERD. Det vill säga, det misslyckades med att hitta tecken på GERD hos många patienter som hade GERD eftersom patienterna hade liten eller ingen skada på slemhinnan i matstrupen. Röntgenbilderna kunde bara visa de sällsynta komplikationerna av GERD, till exempel sår och förträngningar. Röntgenstrålar har övergetts som ett sätt att diagnostisera GERD, även om de fortfarande kan vara användbara tillsammans med endoskopi vid utvärdering av komplikationer.
När GERD påverkar halsen eller struphuvudet och orsakar symtom på hosta, heshet eller halsont, besöker patienter ofta en öron-, näs- och halsspecialist. ÖNH-specialisten upptäcker ofta tecken på inflammation i halsen eller struphuvudet. Även om sjukdomar i halsen eller struphuvudet vanligtvis är orsaken till inflammationen, kan ibland GERD vara orsaken. Följaktligen försöker ÖNH-specialister ofta syradämpande behandling för att bekräfta diagnosen GERD. Detta tillvägagångssätt har dock samma problem som diskuterats ovan, som beror på att man använder responsen på behandlingen för att bekräfta GERD.
Esofageal syratestning anses vara en "guldstandard" för att diagnostisera GERD. Som diskuterats tidigare är återflöde av syra vanligt i den allmänna befolkningen. Patienter med symtom eller komplikationer av GERD har dock reflux av mer syra än individer utan symtom eller komplikationer av GERD. Dessutom kan normala individer och patienter med GERD särskiljas måttligt bra från varandra genom den tid som matstrupen innehåller syra.
Mängden tid som matstrupen innehåller syra bestäms av ett test som kallas ett 24-timmars pH-test i matstrupen. (pH är ett matematiskt sätt att uttrycka mängden surhet.) För detta test förs ett litet rör (kateter) genom näsan och placeras i matstrupen. På spetsen av katetern finns en sensor som känner av syra. Den andra änden av katetern går ut från näsan, lindas tillbaka över örat och färdas ner till midjan, där den är fäst vid en brännare. Varje gång sura uppstötningar kommer tillbaka in i matstrupen från magsäcken, stimulerar den sensorn och inspelaren registrerar refluxepisoden. Efter en tidsperiod på 20 till 24 timmar tas katetern bort och registreringen av reflux från brännaren analyseras.
Det finns problem med att använda pH-testning för att diagnostisera GERD. Trots att normala individer och patienter med GERD kan separeras ganska bra på basis av pH-studier är separationen inte perfekt. Därför kommer vissa patienter med GERD att ha normala mängder sura uppstötningar och vissa patienter utan GERD kommer att ha onormala mängder sura uppstötningar. Det kräver något annat än pH-testet för att bekräfta närvaron av GERD, till exempel typiska symtom, svar på behandling eller förekomsten av komplikationer av GERD. GERD kan också med säkerhet diagnostiseras när episoder av halsbränna korrelerar med sura uppstötningar, vilket framgår av syratestning.
pH-testning har andra användningsområden vid hanteringen av GERD än att bara diagnostisera GERD. Testet kan till exempel hjälpa till att avgöra varför GERD-symtom inte svarar på behandlingen. Kanske kommer 10 till 20 procent av patienterna inte att få sina symtom avsevärt förbättrade genom behandling för GERD. Denna brist på svar på behandlingen kan orsakas av ineffektiv behandling. Detta innebär att läkemedlet inte undertrycker produktionen av syra i magen tillräckligt och inte minskar sura uppstötningar. Alternativt kan bristen på svar förklaras av en felaktig diagnos av GERD. I båda dessa situationer kan pH-testet vara mycket användbart. Om testning avslöjar betydande återflöde av syra medan medicineringen fortsätter, är behandlingen ineffektiv och kommer att behöva ändras. Om testning avslöjar bra syraundertryckande med minimalt återflöde av syra, är diagnosen GERD sannolikt felaktig och andra orsaker till symtomen måste sökas.
pH-testning kan också användas för att utvärdera om reflux är orsaken till symtom (vanligtvis halsbränna). För att göra denna utvärdering, medan 24-timmars ph-testning görs, registrerar patienter varje gång de har symtom. Sedan, när testet analyseras, kan det fastställas om sura uppstötningar inträffade vid tidpunkten för symtomen. Om reflux inträffade samtidigt som symtomen, är reflux sannolikt orsaken till symtomen. Om det inte fanns någon reflux vid tidpunkten för symtomen, är det osannolikt att reflux är orsaken till symtomen.
Slutligen kan pH-testning användas för att utvärdera patienter före endoskopisk eller kirurgisk behandling för GERD. Som diskuterats ovan kommer cirka 20 % av patienterna att få en minskning av sina symtom trots att de inte har GERD (placeboeffekten). Före endoskopisk eller kirurgisk behandling är det viktigt att identifiera dessa patienter eftersom de sannolikt inte kommer att dra nytta av behandlingarna. pH-studien kan användas för att identifiera dessa patienter eftersom de kommer att ha normala mängder sura uppstötningar.
A newer method for prolonged measurement (48 hours) of acid exposure in the esophagus utilizes a small, wireless capsule that is attached to the esophagus just above the LES. The capsule is passed to the lower esophagus by a tube inserted through either the mouth or the nose. After the capsule is attached to the esophagus, the tube is removed. The capsule measures the acid refluxing into the esophagus and transmits this information to a receiver that is worn at the waist. After the study, usually after 48 hours, the information from the receiver is downloaded into a computer and analyzed. The capsule falls off of the esophagus after 3-5 days and is passed in the stool. (The capsule is not reused.)
The advantage of the capsule over standard pH testing is that there is no discomfort from a catheter that passes through the throat and nose. Moreover, with the capsule, patients look normal (they don't have a catheter protruding from their noses) and are more likely to go about their daily activities, for example, go to work, without feeling self-conscious. Because the capsule records for a longer period than the catheter (48 versus 24 hours), more data on acid reflux and symptoms are obtained. Nevertheless, it is not clear whether obtaining additional information is important.
Capsule pH testing is expensive. Sometimes the capsule does not attach to the esophagus or falls off prematurely. For periods of time the receiver may not receive signals from the capsule, and some of the information about reflux of acid may be lost. Occasionally there is pain with swallowing after the capsule has been placed, and the capsule may need to be removed endoscopically. Use of the capsule is an exciting use of new technology although it has its own specific problems.
Esophageal motility testing determines how well the muscles of the esophagus are working. For motility testing, a thin tube (catheter) is passed through a nostril, down the back of the throat, and into the esophagus. On the part of the catheter that is inside the esophagus are sensors that sense pressure. A pressure is generated within the esophagus that is detected by the sensors on the catheter when the muscle of the esophagus contracts. The end of the catheter that protrudes from the nostril is attached to a recorder that records the pressure. During the test, the pressure at rest and the relaxation of the lower esophageal sphincter are evaluated. The patient then swallows sips of water to evaluate the contractions of the esophagus.
Esophageal motility testing has two important uses in evaluating GERD. The first is in evaluating symptoms that do not respond to treatment for GERD since the abnormal function of the esophageal muscle sometimes causes symptoms that resemble the symptoms of GERD. Motility testing can identify some of these abnormalities and lead to a diagnosis of an esophageal motility disorder. The second use is evaluation prior to surgical or endoscopic treatment for GERD. In this situation, the purpose is to identify patients who also have motility disorders of the esophageal muscle. The reason for this is that in patients with motility disorders, some surgeons will modify the type of surgery they perform for GERD.
Gastric emptying studies are studies that determine how well food empties from the stomach. As discussed above, about 20 % of patients with GERD have slow emptying of the stomach that may be contributing to the reflux of acid. For gastric emptying studies, the patient eats a meal that is labeled with a radioactive substance. A sensor that is similar to a Geiger counter is placed over the stomach to measure how quickly the radioactive substance in the meal empties from the stomach.
Information from the emptying study can be useful for managing patients with GERD. For example, if a patient with GERD continues to have symptoms despite treatment with the usual medications, doctors might prescribe other medications that speed-up emptying of the stomach. Alternatively, in conjunction with GERD surgery, they might do a surgical procedure that promotes a more rapid emptying of the stomach. Nevertheless, it is still debated whether a finding of reduced gastric emptying should prompt changes in the surgical treatment of GERD.
Symptoms of nausea, vomiting, and regurgitation may be due either to abnormal gastric emptying or GERD. An evaluation of gastric emptying, therefore, may be useful in identifying patients whose symptoms are due to abnormal emptying of the stomach rather than to GERD.
The acid perfusion (Bernstein) test is used to determine if chest pain is caused by acid reflux. For the acid perfusion test, a thin tube is passed through one nostril, down the back of the throat, and into the middle of the esophagus. A dilute, acid solution and a physiologic salt solution (similar to the fluid that bathes the body's cells) are alternately poured (perfused) through the catheter and into the esophagus. The patient is unaware of which solution is being infused. If the perfusion with acid provokes the patient's usual pain and perfusion of the salt solution produces no pain, it is likely that the patient's pain is caused by acid reflux.
The acid perfusion test, however, is used only rarely. A better test for correlating pain and acid reflux is a 24-hour esophageal pH or pH capsule study during which patients note when they are having pain. It then can be determined from the pH recording if there was an episode of acid reflux at the time of the pain. This is the preferable way of deciding if acid reflux is causing a patient's pain. It does not work well, however, for patients who have infrequent pain, for example every two to three days, which may be missed by a one or two day pH study. In these cases, an acid perfusion test may be reasonable.
One of the simplest treatments for GERD is referred to as life-style changes, a combination of several changes in habit, particularly related to eating.
As discussed above, reflux of acid is more injurious at night than during the day. At night, when individuals are lying down, it is easier for reflux to occur. The reason that it is easier is because gravity is not opposing the reflux, as it does in the upright position during the day. In addition, the lack of an effect of gravity allows the refluxed liquid to travel further up the esophagus and remain in the esophagus longer. These problems can be overcome partially by elevating the upper body in bed. The elevation is accomplished either by putting blocks under the bed's feet at the head of the bed or, more conveniently, by sleeping with the upper body on a foam rubber wedge. These maneuvers raise the esophagus above the stomach and partially restore the effects of gravity. It is important that the upper body and not just the head be elevated. Elevating only the head does not raise the esophagus and fails to restore the effects of gravity.
Elevation of the upper body at night generally is recommended for all patients with GERD. Nevertheless, most patients with GERD have reflux only during the day and elevation at night is of little benefit for them. It is not possible to know for certain which patients will benefit from elevation at night unless acid testing clearly demonstrates night reflux. However, patients who have heartburn, regurgitation, or other symptoms of GERD at night are probably experiencing reflux at night and definitely should elevate their upper body when sleeping. Reflux also occurs less frequently when patients lie on their left rather than their right sides.
Several changes in eating habits can be beneficial in treating GERD. Reflux is worse following meals. This probably is so because the stomach is distended with food at that time and transient relaxations of the lower esophageal sphincter are more frequent. Therefore, smaller and earlier evening meals may reduce the amount of reflux for two reasons. First, the smaller meal results in lesser distention of the stomach. Second, by bedtime, a smaller and earlier meal is more likely to have emptied from the stomach than is a larger one. As a result, reflux is less likely to occur when patients with GERD lie down to sleep.
Certain foods are known to reduce the pressure in the lower esophageal sphincter and thereby promote reflux. These foods should be avoided and include:
Fatty foods (which should be decreased) and smoking (which should be stopped) also reduce the pressure in the sphincter and promote reflux.
In addition, patients with GERD may find that other foods aggravate their symptoms. Examples are spicy or acid-containing foods, like citrus juices, carbonated beverages, and tomato juice. These foods should also be avoided if they provoke symptoms.
One novel approach to the treatment of GERD is chewing gum. Chewing gum stimulates the production of more bicarbonate-containing saliva and increases the rate of swallowing. After the saliva is swallowed, it neutralizes acid in the esophagus. In effect, chewing gum exaggerates one of the normal processes that neutralize acid in the esophagus. It is not clear, however, how effective chewing gum is in treating heartburn. Nevertheless, chewing gum after meals is certainly worth a try.
There is a variety of over-the-counter (for example, antacids and foam barriers) and prescription medications (for example, proton pump inhibitors, histamine antagonists, and promotility drugs) for treating GERD.
Despite the development of potent medications for the treatment of GERD, antacids remain a mainstay of treatment. Antacids neutralize the acid in the stomach so that there is no acid to reflux. The problem with antacids is that their action is brief. They are emptied from the empty stomach quickly, in less than an hour, and the acid then re-accumulates. The best way to take antacids, therefore, is approximately one hour after meals, which is just before the symptoms of reflux begin after a meal. Since the food from meals slows the emptying from the stomach, an antacid taken after a meal stays in the stomach longer and is effective longer. For the same reason, a second dose of antacids approximately two hours after a meal takes advantage of the continuing post-meal slower emptying of the stomach and replenishes the acid-neutralizing capacity within the stomach.
Antacids may be aluminum, magnesium, or calcium-based. Calcium-based antacids (usually calcium carbonate), unlike other antacids, stimulate the release of gastrin from the stomach and duodenum. Gastrin is the hormone that is primarily responsible for the stimulation of acid secretion by the stomach. Therefore, the secretion of acid rebounds after the direct acid-neutralizing effect of the calcium carbonate is exhausted. The rebound is due to the release of gastrin, which results in an overproduction of acid. Theoretically at least, this increased acid is not good for GERD.
Acid rebound, however, is not clinically important. That is, treatment with calcium carbonate is not less effective or safe than treatment with antacids not containing calcium carbonate. Nevertheless, the phenomenon of acid rebound is theoretically harmful. In practice, therefore, calcium-containing antacids such as Tums and Rolaids are not recommended for frequent use. The occasional use of these calcium carbonate-containing antacids, however, is not believed to be harmful. The advantages of calcium carbonate-containing antacids are their low cost, the calcium they add to the diet, and their convenience as compared to liquids.
Aluminum-containing antacids tend to cause constipation, while magnesium-containing antacids tend to cause diarrhea. If diarrhea or constipation becomes a problem, it may be necessary to switch antacids, or use antacids containing both aluminum and magnesium.
Although antacids can neutralize acid, they do so for only a short period. For substantial neutralization of acid throughout the day, antacids would need to be given frequently, at least every hour.
The first medication developed for the more effective and convenient treatment of acid-related diseases, including GERD, was a histamine antagonist, specifically cimetidine (Tagamet). Histamine is an important chemical because it stimulates acid production by the stomach. Released within the wall of the stomach, histamine attaches to receptors (binders) on the stomach's acid-producing cells and stimulates the cells to produce acid. Histamine antagonists work by blocking the receptor for histamine and thereby preventing histamine from stimulating the acid-producing cells. (Histamine antagonists are referred to as H2 antagonists because the specific receptor they block is the histamine type 2 receptor.)
As histamine is particularly important for the stimulation of acid after meals, H2 antagonists are best taken 30 minutes before meals. The reason for this timing is so that the H2 antagonists will be at peak levels in the body after the meal when the stomach is actively producing acid. H2 antagonists also can be taken at bedtime to suppress the nighttime production of acid.
H2 antagonists are very good for relieving the symptoms of GERD, particularly heartburn. However, they are not very good for healing the inflammation (esophagitis) that may accompany GERD. They are used primarily for the treatment of heartburn in GERD that is not associated with inflammation or complications, such as erosions or ulcers, strictures, or Barrett's esophagus.
Three different H2 antagonists are available by prescription, including cimetidine (Tagamet), nizatidine (Axid), and famotidine (Pepcid). Two of these, cimetidine (Tagamet HB) and famotidine (Pepcid AC, Zantac 360) are available over-the-counter (OTC), without the need for a prescription. However, the OTC dosages are lower than those available by prescription.
The second type of drug developed specifically for acid-related diseases, such as GERD, was a proton pump inhibitor (PPI), specifically, omeprazole (Prilosec). A PPI blocks the secretion of acid into the stomach by the acid-secreting cells. The advantage of a PPI over an H2 antagonist is that the PPI shuts off acid production more completely and for a longer period of time. Not only is the PPI good for treating the symptom of heartburn, but it also is good for protecting the esophagus from acid so that esophageal inflammation can heal.
PPIs are used when H2 antagonists do not relieve symptoms adequately or when complications of GERD such as erosions or ulcers, strictures, or Barrett's esophagus exist. Five different PPIs are approved for the treatment of GERD, including omeprazole (Prilosec, Dexilant), lansoprazole (Prevacid), rabeprazole (Aciphex), pantoprazole (Protonix), and esomeprazole (Nexium), and dexlansoprazole (Dexilant). A sixth PPI product consists of a combination of omeprazole and sodium bicarbonate (Zegerid). PPIs (except for Zegerid) are best taken an hour before meals. The reason for this timing is that the PPIs work best when the stomach is most actively producing acid, which occurs after meals. If the PPI is taken before the meal, it is at peak levels in the body after the meal when the acid is being made.
Pro-motility drugs work by stimulating the muscles of the gastrointestinal tract, including the esophagus, stomach, small intestine, and/or colon. One pro-motility drug, metoclopramide (Reglan), is approved for GERD. Pro-motility drugs increase the pressure in the lower esophageal sphincter and strengthen the contractions (peristalsis) of the esophagus. Both effects would be expected to reduce the reflux of acid. However, these effects on the sphincter and esophagus are small. Therefore, it is believed that the primary effect of metoclopramide may be to speed up emptying of the stomach, which also would be expected to reduce reflux.
Pro-motility drugs are most effective when taken 30 minutes before meals and again at bedtime. They are not very effective for treating either the symptoms or complications of GERD. Therefore, the pro-motility agents are reserved either for patients who do not respond to other treatments or are added to enhance other treatments for GERD.
Foam barriers provide a unique form of treatment for GERD. Foam barriers are tablets that are composed of an antacid and a foaming agent. As the tablet disintegrates and reaches the stomach, it turns into foam that floats on top of the liquid contents of the stomach. The foam forms a physical barrier to the reflux of liquid. At the same time, the antacid bound to the foam neutralizes acid that comes into contact with the foam. The tablets are best taken after meals (when the stomach is distended) and when lying down, both times when reflux is more likely to occur. Foam barriers are not often used as the first or only treatment for GERD. Rather, they are added to other drugs for GERD when the other drugs are not adequately effective in relieving symptoms. There is only one foam barrier, which is a combination of aluminum hydroxide gel, magnesium trisilicate, and alginate (Gaviscon).
The drugs described above usually are effective in treating the symptoms and complications of GERD. Nevertheless, sometimes they are not. For example, despite adequate suppression of acid and relief from heartburn, regurgitation, with its potential for complications in the lungs, may still occur. Moreover, the amounts and/or numbers of drugs that are required for satisfactory treatment are sometimes so great that drug treatment is unreasonable. In such situations, surgery can effectively stop reflux.
The surgical procedure that is done to prevent reflux is technically known as fundoplication and is called reflux surgery or anti-reflux surgery. During fundoplication, any hiatal hernial sac is pulled below the diaphragm and stitched there. In addition, the opening in the diaphragm through which the esophagus passes is tightened around the esophagus. Finally, the upper part of the stomach next to the opening of the esophagus into the stomach is wrapped around the lower esophagus to make an artificial lower esophageal sphincter. All of this surgery can be done through an incision in the abdomen (laparotomy) or using a technique called laparoscopy. During laparoscopy, a small viewing device and surgical instruments are passed through several small puncture sites in the abdomen. This procedure avoids the need for a major abdominal incision.
Surgery is very effective at relieving symptoms and treating the complications of GERD. Approximately 80% of patients will have good or excellent relief of their symptoms for at least 5 to 10 years. Nevertheless, many patients who have had surgery will continue to take drugs for reflux. It is not clear whether they take the drugs because they continue to have reflux and symptoms of reflux or if they take them for symptoms that are being caused by problems other than GERD. The most common complication of fundoplication is swallowed food that sticks at the artificial sphincter. Fortunately, the sticking usually is temporary. If it is not transient, endoscopic treatment to stretch (dilate) the artificial sphincter usually will relieve the problem. Only occasionally is it necessary to re-operate to revise the prior surgery.
Very recently, endoscopic techniques for the treatment of GERD have been developed and tested. One type of endoscopic treatment involves suturing (stitching) the area of the lower esophageal sphincter, which essentially tightens the sphincter.
A second type involves the application of radio-frequency waves to the lower part of the esophagus just above the sphincter. The waves cause damage to the tissue beneath the esophageal lining and a scar (fibrosis) forms. The scar shrinks and pulls on the surrounding tissue, thereby tightening the sphincter and the area above it.
A third type of endoscopic treatment involves the injection of materials into the esophageal wall in the area of the LES. The injected material is intended to increase pressure in the LES and thereby prevent reflux. In one treatment the injected material was a polymer. Unfortunately, the injection of polymer led to serious complications, and the material for injection is no longer available. Another treatment involving injection of expandable pellets also was discontinued. Limited information is available about a third type of injection which uses gelatinous polymethylmethacrylate microspheres.
Endoscopic treatment has the advantage of not requiring surgery. It can be performed without hospitalization. Experience with endoscopic techniques is limited. It is not clear how effective they are, especially long-term. Because the effectiveness and the full extent of potential complications of endoscopic techniques are not clear, it is felt generally that endoscopic treatment should only be done as part of experimental trials.
Transient LES relaxations appear to be the most common way in which acid reflux occurs. Although there is an available drug that prevents relaxations (baclofen), it has side effects that are too frequent to be generally useful. Much attention is being directed at the development of drugs that prevent these relaxations without accompanying side effects.
There are several ways to approach the evaluation and management of GERD. The approach depends primarily on the frequency and severity of symptoms, the adequacy of the response to treatment, and the presence of complications.
For infrequent heartburn, the most common symptom of GERD, life-style changes and an occasional antacid may be all that is necessary. If heartburn is frequent, daily non-prescription-strength (over-the-counter) H2 antagonists may be adequate. A foam barrier also can be used with the antacid or H2 antagonist.
If life-style changes and antacids, non-prescription H2 antagonists, and a foam barrier do not adequately relieve heartburn, it is time to see a physician for further evaluation and to consider prescription-strength drugs. The evaluation by the physician should include an assessment for possible complications of GERD based on the presence of such symptoms or findings as:
Clues to the presence of diseases that may mimic GERD, such as gastric or duodenal ulcers and esophageal motility disorders, should be sought.
If there are no symptoms or signs of complications and no suspicion of other diseases, a therapeutic trial of acid suppression with H2 antagonists often is used. If H2 antagonists are not adequately effective, a second trial, with the more potent PPIs, can be given. Sometimes, a trial of treatment begins with a PPI and skips the H2 antagonist. If treatment relieves the symptoms completely, no further evaluation may be necessary and the effective drug, the H2 antagonist or PPI, is continued. As discussed previously, however, there are potential problems with this commonly used approach, and some physicians would recommend a further evaluation for almost all patients they see.
If at the time of evaluation, there are symptoms or signs that suggest complicated GERD or a disease other than GERD or if the relief of symptoms with H2 antagonists or PPIs is not satisfactory, a further evaluation by endoscopy (EGD) definitely should be done.
There are several possible results of endoscopy and each requires a different approach to treatment. If the esophagus is normal and no other diseases are found, the goal of treatment simply is to relieve symptoms. Therefore, prescription strength H2 antagonists or PPIs are appropriate. If damage to the esophagus (esophagitis or ulceration) is found, the goal of treatment is healing the damage. In this case, PPIs are preferred over H2 antagonists because they are more effective for healing.
If complications of GERD, such as stricture or Barrett's esophagus are found, treatment with PPIs also is more appropriate. However, the adequacy of the PPI treatment probably should be evaluated with a 24-hour pH study during treatment with the PPI. (With PPIs, although the amount of acid reflux may be reduced enough to control symptoms, it may still be abnormally high. Therefore, judging the adequacy of suppression of acid reflux by only the response of symptoms to treatment is not satisfactory.) Strictures may also need to be treated by endoscopic dilatation (widening) of the esophageal narrowing. With Barrett's esophagus, periodic endoscopic examination should be done to identify pre-malignant changes in the esophagus.
If symptoms of GERD do not respond to maximum doses of PPI, there are two options for management. The first is to perform 24-hour pH testing to determine whether the PPI is ineffective or if a disease other than GERD is likely to be present. If the PPI is ineffective, a higher dose of PPI may be tried. The second option is to go ahead without 24 hour pH testing and to increase the dose of PPI. Another alternative is to add another drug to the PPI that works in a way that is different from the PPI, for example, a pro-motility drug or a foam barrier. If necessary, all three types of drugs can be used. If there is not a satisfactory response to this maximal treatment, 24 hour pH testing should be done.
Who should consider surgery or, perhaps, an endoscopic treatment trial for GERD? (As mentioned previously, the effectiveness of the recently developed endoscopic treatments remains to be determined.) Patients should consider surgery if they have regurgitation that cannot be controlled with drugs. This recommendation is particularly important if the regurgitation results in infections in the lungs or occurs at night when aspiration into the lungs is more likely. Patients also should consider surgery if they require large doses of PPI or multiple drugs to control their reflux. It is debated whether or not a desire to be free of the need to take life-long drugs to prevent symptoms of GERD is by itself a satisfactory reason for having surgery.
Some physicians - primarily surgeons - recommend that all patients with Barrett's esophagus should have surgery. This recommendation is based on the belief that surgery is more effective than endoscopic surveillance or ablation of the abnormal tissue followed by treatment with acid-suppressing drugs in preventing both the reflux and the cancerous changes in the esophagus. There are no studies, however, demonstrating the superiority of surgery over drugs or ablation for the treatment of GERD and its complications. Moreover, the effectiveness of drug treatment can be monitored with 24 hour pH testing.
One unresolved issue in GERD is the inconsistent relationships among acid reflux, heartburn, and damage to the lining of the esophagus (esophagitis and the complications).
Clearly, we have much to learn about the relationship between acid reflux and esophageal damage, and about the processes (mechanisms) responsible for heartburn. This issue is of more than passing interest. Knowledge of the mechanisms that produce heartburn and esophageal damage raises the possibility of new treatments that would target processes other than acid reflux.
One of the more interesting theories that has been proposed to answer some of these questions involves the reason for pain when acid refluxes. It often is assumed that the pain is caused by irritating acid contacting an inflamed esophageal lining. But the esophageal lining usually is not inflamed. It is possible therefore, that the acid is stimulating the pain nerves within the esophageal wall just beneath the lining. Although this may be the case, a second explanation is supported by the work of one group of scientists. These scientists find that heartburn provoked by acid in the esophagus is associated with contraction of the muscle in the lower esophagus. Perhaps it is the contraction of the muscle that somehow leads to the pain. It also is possible, however, that the contraction is an epiphenomenon, that is, refluxed acid stimulates pain nerves and causes the muscle to contract, but it is not the contraction that causes the pain. More studies will be necessary before the exact mechanism(s) that causes heartburn is clear.
There are potentially injurious agents that can be refluxed other than acid, for example, bile. Until recently it has been impossible or difficult to accurately identify non-acid reflux and, therefore, to study whether or not non-acid reflux is injurious or can cause symptoms.
A new technology allows the accurate determination of non-acid reflux. This technology uses the measurement of impedance changes within the esophagus to identify reflux of liquid, be it acid or non-acid. By combining measurement of impedance and pH it is possible to identify reflux and to tell if the reflux is acid or non-acid. It is too early to know how important non-acid reflux is in causing esophageal damage, symptoms, or complications, but there is little doubt that this new technology will be able to resolve the issues surrounding non-acid reflux.
 Hur avföringspåverkan kan behandlas
Hur avföringspåverkan kan behandlas
 Varför du går ner i vikt efter att ha börjat med SCD och GAPS
Varför du går ner i vikt efter att ha börjat med SCD och GAPS
 Fettlever (Alkoholfri fettlever)
Fettlever (Alkoholfri fettlever)
 CT-skanning vs. MRI-skillnader mellan maskiner, kostnader, användningar
CT-skanning vs. MRI-skillnader mellan maskiner, kostnader, användningar
 Två justeringar för att dominera din matsmältning
Två justeringar för att dominera din matsmältning
 The Rainbow Diet Food Lists by Color:How To Eat The Rainbow Diet
The Rainbow Diet Food Lists by Color:How To Eat The Rainbow Diet
 Akut pankreatit - Diagnos av akut buk
Det finns en uppfattning om att akut pankreatit är en mycket sällsynt sjukdom. Under de senaste två decennierna har en avsevärd ökning av frekvensen av akut pankreatit skisserats, och den måste tydlig
Akut pankreatit - Diagnos av akut buk
Det finns en uppfattning om att akut pankreatit är en mycket sällsynt sjukdom. Under de senaste två decennierna har en avsevärd ökning av frekvensen av akut pankreatit skisserats, och den måste tydlig
 Vad kan orsaka bäckensmärta hos män?
Vad är bäckensmärta? Orsaker till bäckensmärtor hos män inkluderar cykling, tidigare prostatitinfektioner, kemisk irritation, sexuella övergrepp, bäckenbottenmuskler problem, prostatairritation frå
Vad kan orsaka bäckensmärta hos män?
Vad är bäckensmärta? Orsaker till bäckensmärtor hos män inkluderar cykling, tidigare prostatitinfektioner, kemisk irritation, sexuella övergrepp, bäckenbottenmuskler problem, prostatairritation frå
 Dysbios av den orala mikrobiotan orsakar tarm- och hälsoproblem
Din mun är hem för över 700 olika mikrober, som utgör den orala mikrobiotan. De kan dock påverka din tarm och din allmänna hälsa. Mikroberna i din mun är en viktig del av ett naturligt ekosystem i mu
Dysbios av den orala mikrobiotan orsakar tarm- och hälsoproblem
Din mun är hem för över 700 olika mikrober, som utgör den orala mikrobiotan. De kan dock påverka din tarm och din allmänna hälsa. Mikroberna i din mun är en viktig del av ett naturligt ekosystem i mu