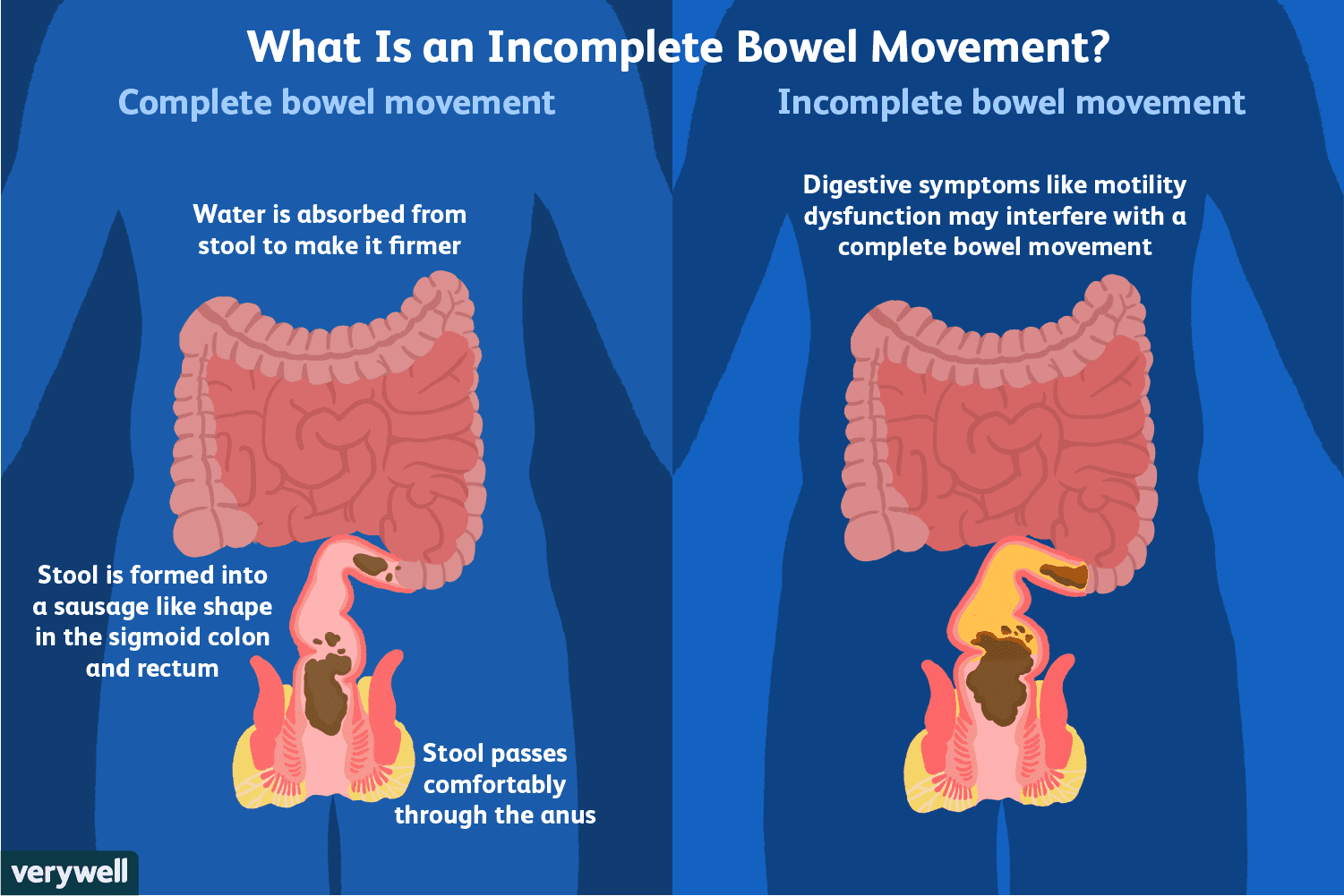
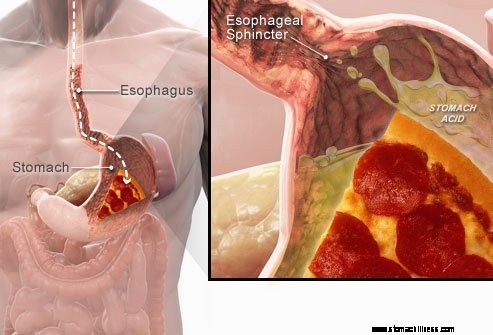
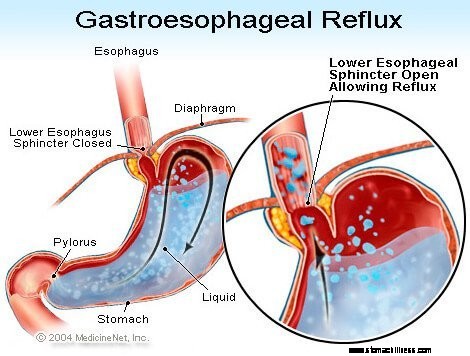
 Als je voedsel doorslikt, gaat het door de slokdarm en passeert het een gespierde ring die bekend staat als de onderste slokdarmsfincter ( LE). Deze structuur gaat open om voedsel in de maag te laten komen. Het wordt verondersteld gesloten te blijven om de maaginhoud te houden waar ze hoort.
Als je voedsel doorslikt, gaat het door de slokdarm en passeert het een gespierde ring die bekend staat als de onderste slokdarmsfincter ( LE). Deze structuur gaat open om voedsel in de maag te laten komen. Het wordt verondersteld gesloten te blijven om de maaginhoud te houden waar ze hoort.
GERD of zure reflux symptomen worden veroorzaakt door de regurgitatie van zure vloeibare maaginhoud terug in de slokdarm. Het meest voorkomende symptoom van GERD is brandend maagzuur.
Andere symptomen die kunnen optreden als gevolg van GERD zijn:
 Het meest voorkomende symptoom van GERD is brandend maagzuur.
Het meest voorkomende symptoom van GERD is brandend maagzuur. Gastro-oesofageale refluxziekte, gewoonlijk GERD of zure reflux genoemd, is een aandoening waarbij de vloeistofinhoud van de maag terugvloeit (terugvloeit of terugvloeit) in de slokdarm. De vloeistof kan het slijmvlies ontsteken en beschadigen (oesofagitis), hoewel bij een minderheid van de patiënten zichtbare tekenen van ontsteking optreden. De uitgebraakte vloeistof bevat meestal zuur en pepsine die door de maag worden geproduceerd. (Pepsine is een enzym dat de vertering van eiwitten in de maag begint.) De terugvloeiende vloeistof kan ook gal bevatten die vanuit de twaalfvingerige darm in de maag is terechtgekomen. Het eerste deel van de dunne darm dat aan de maag vastzit. Aangenomen wordt dat zuur het meest schadelijke bestanddeel van de terugvloeiende vloeistof is. Pepsine en gal kunnen ook de slokdarm beschadigen, maar hun rol bij de productie van slokdarmontsteking en -beschadiging is niet zo duidelijk als de rol van zuur.
GERD is een chronische aandoening. Als het eenmaal begint, is het meestal levenslang. Als er een verwonding is aan het slijmvlies van de slokdarm (oesofagitis), is dit ook een chronische aandoening. Bovendien zal het letsel bij de meeste patiënten binnen enkele maanden terugkeren nadat de slokdarm is genezen met de behandeling en de behandeling wordt stopgezet. Zodra de behandeling voor GERD is begonnen, moet deze echter voor onbepaalde tijd worden voortgezet. Sommige patiënten met intermitterende symptomen en geen oesofagitis kunnen echter alleen tijdens symptomatische perioden worden behandeld.
In feite komt reflux van de vloeibare inhoud van de maag in de slokdarm voor bij de meeste normale personen. Eén studie toonde aan dat reflux vaak voorkomt bij normale personen en bij patiënten met GERD. Bij patiënten met GERD bevat de refluxvloeistof echter vaker zuur en blijft het zuur langer in de slokdarm. Er is ook gevonden dat vloeistof terugvloeit naar een hoger niveau in de slokdarm bij patiënten met GERD dan bij normale personen.
Zoals vaak het geval is, heeft het lichaam manieren om zichzelf te beschermen tegen de schadelijke effecten van reflux en zuur. De meeste reflux treedt bijvoorbeeld overdag op wanneer mensen rechtop staan. In rechtopstaande positie is de kans groter dat de teruggevloeide vloeistof terugstroomt in de maag vanwege het effect van de zwaartekracht. Bovendien, terwijl individuen wakker zijn, slikken ze herhaaldelijk, ongeacht of er reflux is of niet. Elke slik brengt eventuele terugvloeiende vloeistof terug in de maag. Ten slotte produceren de speekselklieren in de mond speeksel, dat bicarbonaat bevat. Bij elke slik reist bicarbonaathoudend speeksel door de slokdarm. Het bicarbonaat neutraliseert de kleine hoeveelheid zuur die in de slokdarm achterblijft nadat de zwaartekracht en het slikken het grootste deel van de zure vloeistof heeft verwijderd.
Zwaartekracht, slikken en speeksel zijn belangrijke beschermende mechanismen voor de slokdarm, maar ze zijn alleen effectief als personen rechtop staan. 'S Nachts tijdens de slaap heeft de zwaartekracht geen effect, stopt het slikken en wordt de afscheiding van speeksel verminderd. Daarom is de kans groter dat reflux die 's nachts optreedt, ertoe leidt dat zuur langer in de slokdarm blijft en grotere schade aan de slokdarm veroorzaakt.
Bepaalde aandoeningen maken een persoon vatbaar voor GERD. GERD kan bijvoorbeeld een ernstig probleem zijn tijdens de zwangerschap. De verhoogde hormoonspiegels van de zwangerschap veroorzaken waarschijnlijk reflux door de druk in de onderste slokdarmsfincter te verlagen (zie hieronder). Tegelijkertijd verhoogt de groeiende foetus de druk in de buik. Van beide effecten zou worden verwacht dat ze de reflux verhogen. Ook zijn patiënten met ziekten die de slokdarmspieren verzwakken, zoals sclerodermie of gemengde bindweefselaandoeningen, vatbaarder voor het ontwikkelen van GERD.
De oorzaak van GERD is complex en kan meerdere oorzaken hebben. Bovendien kunnen verschillende oorzaken verschillende individuen treffen of zelfs bij hetzelfde individu op verschillende tijdstippen. Een klein aantal patiënten met GERD produceert abnormaal grote hoeveelheden zuur, maar dit komt niet vaak voor en draagt bij de overgrote meerderheid van de patiënten niet bij.
De factoren die bijdragen aan GERD zijn:
De werking van de onderste slokdarmsfincter (LES) is misschien wel de belangrijkste factor (mechanisme) om reflux te voorkomen. De slokdarm is een gespierde buis die zich uitstrekt van de onderste keel naar de maag. De LES is een gespecialiseerde spierring die het onderste uiteinde van de slokdarm omringt, waar deze samenkomt met de maag. De spier waaruit de LES bestaat, is het grootste deel van de tijd actief, dat wil zeggen in rust. Dit betekent dat het samentrekt en de doorgang van de slokdarm naar de maag afsluit. Deze afsluiting van de doorgang voorkomt terugvloeiing. Wanneer voedsel of speeksel wordt ingeslikt, ontspant de LES zich een paar seconden om het voedsel of speeksel van de slokdarm naar de maag te laten gaan, en dan sluit het weer.
Er zijn verschillende afwijkingen van de LES gevonden bij patiënten met GERD. Twee ervan hebben betrekking op de functie van de LES. De eerste is een abnormaal zwakke samentrekking van de LES, waardoor het vermogen om reflux te voorkomen vermindert. De tweede is abnormale relaxaties van de LES, tijdelijke LES-relaxaties genoemd. Ze zijn abnormaal omdat ze geen zwaluwen vergezellen en ze duren lang, tot enkele minuten. Door deze langdurige relaxaties kan reflux gemakkelijker optreden. De voorbijgaande LES-relaxaties komen het meest voor bij patiënten met GERD na de maaltijd wanneer de maag is opgezwollen met voedsel. Voorbijgaande LES-relaxaties komen ook voor bij personen zonder GERD, maar ze komen niet vaak voor.
De meest recent beschreven afwijking bij patiënten met GERD is laxiteit van de LES. Specifiek, vergelijkbare uitzettende druk opent de LES meer bij patiënten met GERD dan bij personen zonder GERD. In theorie zou dit in ieder geval een gemakkelijkere opening van de LES mogelijk maken en/of een grotere terugstroom van zuur in de slokdarm wanneer de LES open is.
Hiatale hernia's dragen bij aan reflux, hoewel de manier waarop ze bijdragen niet duidelijk is. Een meerderheid van de patiënten met GERD heeft hiatale hernia's, maar velen niet. Daarom is het niet nodig om een hiatale hernia te hebben om GERD te hebben. Bovendien hebben veel mensen hiatale hernia's maar hebben ze geen GERD. Het is niet met zekerheid bekend hoe of waarom hiatale hernia's ontstaan.
Normaal gesproken bevindt de LES zich op hetzelfde niveau waar de slokdarm van de borstkas door een kleine opening in het middenrif en in de buik gaat. (Het middenrif is een gespierde, horizontale scheidingswand die de borstkas van de buik scheidt.) Bij een hiatale hernia duwt een klein deel van de bovenbuik dat aan de slokdarm hecht, omhoog door het middenrif. Hierdoor komt een klein deel van de maag en de LES in de borstkas te liggen en ligt de LES niet meer ter hoogte van het middenrif.
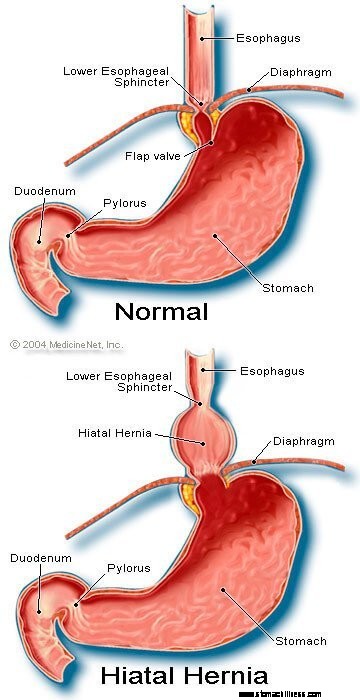 Foto van een hernia Hiatal
Foto van een hernia Hiatal
Het lijkt erop dat het diafragma dat de LES omringt, belangrijk is bij het voorkomen van reflux. Dat wil zeggen, bij personen zonder hiatale hernia's wordt het diafragma rond de slokdarm continu samengetrokken, maar ontspant het vervolgens met slikken, net als de LES. Merk op dat de effecten van de LES en het diafragma op dezelfde locatie optreden bij patiënten zonder hiatale hernia's. Daarom is de barrière tegen reflux gelijk aan de som van de drukken die worden gegenereerd door de LES en het diafragma. Wanneer de LES met een hiatale hernia in de borstkas terechtkomt, blijven het diafragma en de LES hun druk en barrière-effect uitoefenen. Dat doen ze nu echter op verschillende locaties. Bijgevolg zijn de drukken niet langer additief. In plaats daarvan wordt een enkele hogedrukbarrière tegen reflux vervangen door twee barrières met lagere druk, en reflux treedt dus gemakkelijker op. Het verlagen van de drukbarrière is dus een manier waarop een hiatale hernia kan bijdragen aan reflux.
Zoals eerder vermeld, zijn slikken belangrijk bij het elimineren van zuur in de slokdarm. Slikken veroorzaakt een ringvormige samentrekking van de slokdarmspieren, die het lumen (binnenholte) van de slokdarm vernauwt. De samentrekking, aangeduid als peristaltiek, begint in de bovenste slokdarm en gaat naar de onderste slokdarm. Het duwt voedsel, speeksel en al het andere in de slokdarm naar de maag.
Wanneer de samentrekkingsgolf defect is, wordt gerefluxt zuur niet terug in de maag geduwd. Bij patiënten met GERD zijn verschillende contractieafwijkingen beschreven. Het is bijvoorbeeld mogelijk dat de samentrekkingsgolven niet na elke slikken beginnen of dat de samentrekkingsgolven uitsterven voordat ze de maag bereiken. Ook kan de druk die door de weeën wordt gegenereerd, te zwak zijn om het zuur terug in de maag te duwen. Dergelijke afwijkingen van contractie, die de klaring van zuur uit de slokdarm verminderen, worden vaak gevonden bij patiënten met GERD. In feite worden ze het vaakst gevonden bij die patiënten met de meest ernstige GERD. De effecten van abnormale samentrekkingen van de slokdarm zijn naar verwachting 's nachts erger wanneer de zwaartekracht niet helpt om het terugvloeiende zuur naar de maag terug te brengen. Merk op dat roken ook de klaring van zuur uit de slokdarm aanzienlijk vermindert. Dit effect houdt minimaal 6 uur aan na de laatste sigaret.
De meeste reflux gedurende de dag treedt op na de maaltijd. Deze reflux is waarschijnlijk te wijten aan voorbijgaande LES-relaxaties die worden veroorzaakt door uitzetting van de maag met voedsel. Bij een minderheid van de patiënten met GERD is vastgesteld dat ze een maag hebben die abnormaal langzaam leegloopt na een maaltijd. Dit wordt gastroparese genoemd. De langzamere maaglediging verlengt de uitzetting van de maag met voedsel na de maaltijd. Daarom verlengt de langzamere lediging de periode waarin reflux waarschijnlijker is. Er zijn verschillende medicijnen die in verband worden gebracht met een verstoorde maaglediging, zoals:
Individuen mogen niet stoppen met het gebruik van deze of andere medicijnen die zijn voorgeschreven totdat de voorschrijvende arts de mogelijke GERD-situatie met hen heeft besproken.
De symptomen van ongecompliceerde GERD zijn voornamelijk:
Andere symptomen treden op wanneer er complicaties zijn van GERD en zullen met de complicaties worden besproken.
Wanneer zure reflux terugvloeit in de slokdarm bij patiënten met GERD, worden zenuwvezels in de slokdarm gestimuleerd. Deze zenuwstimulatie resulteert meestal in brandend maagzuur, de pijn die kenmerkend is voor GERD. Maagzuur wordt meestal beschreven als een brandende pijn in het midden van de borstkas. Het kan hoog in de buik beginnen of zich uitstrekken tot in de nek. Bij sommige patiënten kan de pijn echter scherp of drukachtig zijn, in plaats van brandend. Dergelijke pijn kan hartpijn (angina pectoris) nabootsen. Bij andere patiënten kan de pijn zich uitstrekken tot in de rug.
Aangezien zure reflux vaker voorkomt na de maaltijd, komt brandend maagzuur vaker voor na de maaltijd. Maagzuur komt ook vaker voor wanneer mensen gaan liggen, omdat zonder de effecten van de zwaartekracht reflux gemakkelijker optreedt en het zuur langzamer naar de maag wordt teruggevoerd. Veel patiënten met GERD worden uit hun slaap gewekt door brandend maagzuur.
Afleveringen van brandend maagzuur komen regelmatig voor. Dit betekent dat de episodes frequenter of ernstiger zijn gedurende een periode van enkele weken of maanden, en dan minder frequent of ernstig worden of zelfs enkele weken of maanden afwezig zijn. Deze periodiciteit van symptomen vormt de grondgedachte voor intermitterende behandeling bij patiënten met GORZ die geen oesofagitis hebben. Desalniettemin is brandend maagzuur een levenslang probleem en komt het bijna altijd terug.
Regurgitatie is het verschijnen van terugvloeiende vloeistof in de mond. Bij de meeste patiënten met GERD bereiken gewoonlijk slechts kleine hoeveelheden vloeistof de slokdarm en blijft de vloeistof in de onderste slokdarm. Af en toe bij sommige patiënten met GERD, worden grotere hoeveelheden vloeistof, soms met voedsel, gerefluxt en bereiken de bovenste slokdarm.
Aan het bovenste uiteinde van de slokdarm bevindt zich de bovenste slokdarmsfincter (UES). De UES is een cirkelvormige spierring die erg lijkt op de LES. Dat wil zeggen, de UES voorkomt dat de inhoud van de slokdarm terugstroomt in de keel. Wanneer kleine hoeveelheden refluxvloeistof en/of voedsel voorbij de UES komen en in de keel komen, kan er een zure smaak in de mond zijn. Als grotere hoeveelheden de UES overschrijden, kunnen patiënten plotseling merken dat hun mond gevuld is met de vloeistof of het voedsel. Bovendien kan frequente of langdurige regurgitatie leiden tot door zuur veroorzaakte erosies van de tanden.
Misselijkheid komt niet vaak voor bij GERD. Bij sommige patiënten kan het echter frequent of ernstig zijn en tot braken leiden. Bij patiënten met onverklaarbare misselijkheid en/of braken is GERD zelfs een van de eerste aandoeningen waarmee rekening moet worden gehouden. Het is niet duidelijk waarom sommige patiënten met GERD voornamelijk brandend maagzuur ontwikkelen en anderen voornamelijk misselijkheid.
De vloeistof uit de maag die terugvloeit in de slokdarm beschadigt de cellen die de slokdarm bekleden. Het lichaam reageert zoals het gewoonlijk reageert op schade, namelijk met een ontsteking (oesofagitis). Het doel van een ontsteking is om de schadelijke stof te neutraliseren en het genezingsproces te starten. Als de schade diep in de slokdarm doordringt, ontstaat er een zweer. Een maagzweer is gewoon een breuk in het slijmvlies van de slokdarm die optreedt in een gebied van ontsteking. Zweren en de extra ontsteking die ze veroorzaken, kunnen eroderen in de bloedvaten van de slokdarm en aanleiding geven tot bloedingen in de slokdarm.
Soms is de bloeding ernstig en kan het volgende nodig zijn:
Zweren van de slokdarm genezen met de vorming van littekens (fibrose). Na verloop van tijd krimpt het littekenweefsel en vernauwt het lumen (binnenholte) van de slokdarm. Deze littekenvernauwing wordt een strictuur genoemd. Doorgeslikt voedsel kan vast komen te zitten in de slokdarm zodra de vernauwing ernstig genoeg wordt (meestal wanneer het slokdarmlumen wordt beperkt tot een diameter van één centimeter). Deze situatie kan endoscopische verwijdering van het vastzittende voedsel noodzakelijk maken. Om te voorkomen dat voedsel blijft plakken, moet de vernauwing vervolgens worden uitgerekt (verbreed). Om herhaling van de strictuur te voorkomen, moet bovendien ook reflux worden voorkomen.
Langdurige en/of ernstige GERD veroorzaakt bij sommige patiënten veranderingen in de cellen die de slokdarm bekleden. Deze cellen zijn voorstadia van kanker en kunnen, hoewel meestal, kanker worden. Deze aandoening wordt de Barrett-slokdarm genoemd en komt voor bij ongeveer 10% van de patiënten met GERD. Het type slokdarmkanker geassocieerd met Barrett-slokdarm (adenocarcinoom) neemt in frequentie toe. Het is niet duidelijk waarom sommige patiënten met GERD de slokdarm van Barrett ontwikkelen, maar de meeste niet.
Barrett's slokdarm kan visueel worden herkend op het moment van een endoscopie en worden bevestigd door microscopisch onderzoek van de voeringcellen. Vervolgens kunnen patiënten met Barrett-slokdarm periodieke surveillance-endoscopieën met biopsieën ondergaan, hoewel er geen overeenstemming is over welke patiënten surveillance nodig hebben. Het doel van surveillance is om de progressie van pre-kanker naar meer kankerachtige veranderingen te detecteren, zodat een kankervoorkomende behandeling kan worden gestart. Er wordt ook aangenomen dat patiënten met Barrett-slokdarm maximale behandeling voor GERD moeten krijgen om verdere schade aan de slokdarm te voorkomen. Procedures worden bestudeerd die de abnormale voeringcellen verwijderen. Er kunnen verschillende endoscopische, niet-chirurgische technieken worden gebruikt om de cellen te verwijderen. Deze technieken zijn aantrekkelijk omdat ze geen operatie vereisen; er zijn echter complicaties en de effectiviteit van de behandelingen op lange termijn is nog niet vastgesteld. Chirurgische verwijdering van de slokdarm is altijd een optie.
Veel zenuwen bevinden zich in de onderste slokdarm. Sommige van deze zenuwen worden gestimuleerd door het terugvloeiende zuur en deze stimulatie resulteert in pijn (meestal brandend maagzuur). Andere zenuwen die worden gestimuleerd, veroorzaken geen pijn. In plaats daarvan stimuleren ze nog andere zenuwen die hoesten veroorzaken. Op deze manier kan refluxvloeistof hoesten veroorzaken zonder ooit de keel te bereiken! Op een vergelijkbare manier kan reflux in de onderste slokdarm de slokdarmzenuwen stimuleren die verbinding maken met en zenuwen kan stimuleren die naar de longen gaan. Deze zenuwen naar de longen kunnen er vervolgens voor zorgen dat de kleinere ademhalingsbuizen vernauwen, wat resulteert in een astma-aanval.
Hoewel GERD hoest kan veroorzaken, is het geen veelvoorkomende oorzaak van onverklaarbaar hoesten. Hoewel GERD ook een oorzaak van astma kan zijn, is het waarschijnlijker dat het astma-aanvallen veroorzaakt bij patiënten die al astma hebben. Hoewel chronische hoest en astma veelvoorkomende kwalen zijn, is het niet duidelijk hoe vaak ze verergeren of veroorzaakt worden door GERD.
Als refluxvloeistof voorbij de bovenste slokdarmsfincter komt, kan het de keel (farynx) en zelfs de strottenhoofd (strottenhoofd) binnendringen. De resulterende ontsteking kan leiden tot keelpijn en heesheid. Net als bij hoesten en astma is het niet duidelijk hoe vaak GERD verantwoordelijk is voor een anders onverklaarbare ontsteking van de keel en het strottenhoofd.
Terugvloeiende vloeistof die van de keel (farynx) naar het strottenhoofd gaat, kan de longen binnendringen (aspiratie). De terugvloeiing van vloeistof in de longen (aspiratie genoemd) resulteert vaak in hoesten en verstikking. Aspiratie kan echter ook optreden zonder deze symptomen te veroorzaken. Met of zonder deze symptomen kan aspiratie leiden tot infectie van de longen en leiden tot longontsteking. Dit type longontsteking is een ernstig probleem dat onmiddellijke behandeling vereist. Wanneer aspiratie niet gepaard gaat met symptomen, kan dit leiden tot langzame, progressieve littekens in de longen (pulmonale fibrose) die te zien zijn op röntgenfoto's van de borst. Aspiratie is waarschijnlijker 's nachts, omdat dan de processen (mechanismen) die beschermen tegen reflux niet actief zijn en de hoestreflex die de longen beschermt ook niet actief is.
De keel communiceert met de neusholtes. Bij kleine kinderen bevinden zich twee stukken lymfeweefsel, de adenoïden genaamd, waar het bovenste deel van de keel aansluit op de neusholtes. De passages van de sinussen en de buizen van de middenoren (buisjes van Eustachius) monden uit in de achterkant van de neusholtes nabij de adenoïden. Terugvloeiende vloeistof die de bovenste keel binnendringt, kan de adenoïden doen ontsteken en ze doen opzwellen. De gezwollen amandelen kunnen dan de doorgangen van de sinussen en de buis van Eustachius blokkeren. Wanneer de sinussen en middenoren worden afgesloten van de neusholtes door de zwelling van de adenoïden, hoopt zich daarin vocht op. Deze ophoping van vocht kan leiden tot ongemak in de sinussen en oren. Aangezien de adenoïden prominent aanwezig zijn bij jonge kinderen, en niet bij volwassenen, wordt deze vochtophoping in de oren en sinussen gezien bij kinderen en niet bij volwassenen.
Er zijn verschillende procedures, tests en evaluatie van symptomen (bijvoorbeeld brandend maagzuur) om patiënten met GERD te diagnosticeren en te evalueren.
De gebruikelijke manier waarop GERD is door zijn karakteristieke symptoom, brandend maagzuur. Brandend maagzuur wordt het vaakst beschreven als een substernale (onder het midden van de borst) verbranding die optreedt na de maaltijd en vaak verergert bij het liggen. Om de diagnose te bevestigen, behandelen artsen patiënten vaak met medicijnen om de maagzuurproductie te onderdrukken. Als het brandend maagzuur dan grotendeels is afgenomen, wordt de diagnose GERD als bevestigd beschouwd. Deze benadering van het stellen van een diagnose op basis van een respons van de symptomen op de behandeling wordt gewoonlijk een therapeutisch onderzoek genoemd.
Er zijn problemen met deze benadering. Patiënten met aandoeningen die GERD kunnen nabootsen, met name duodenum- of maag- (maag)zweren, kunnen bijvoorbeeld ook daadwerkelijk op een dergelijke behandeling reageren. Als de arts in deze situatie aanneemt dat het probleem GORZ is, wordt de oorzaak van de zweerziekte over het hoofd gezien, zoals een type infectie genaamd Helicobacter pylori (H. pylori ), of niet-steroïde anti-inflammatoire geneesmiddelen of NSAID's (bijvoorbeeld ibuprofen), kunnen ook zweren veroorzaken en deze aandoeningen zouden anders worden behandeld dan GERD.
Bovendien is er, zoals bij elke behandeling, misschien een placebo-effect van 20%, wat betekent dat 20% van de patiënten zal reageren op een placebo (inactieve) pil of, inderdaad, op elke behandeling. Dit betekent dat 20% van de patiënten die andere oorzaken van hun symptomen hebben dan GERD (of zweren), een afname van hun symptomen zullen hebben na behandeling voor GERD. Op basis van hun respons op de behandeling (de therapeutische studie) zullen deze patiënten dus verder worden behandeld voor GERD, ook al hebben ze geen GERD. Bovendien zal de ware oorzaak van hun symptomen niet worden onderzocht.
Bovenste gastro-intestinale endoscopie (ook bekend als esophago-gastro-duodenoscopie of EGD) is een veel voorkomende manier om GERD te diagnosticeren. EGD is een procedure waarbij een buisje met een optisch systeem voor visualisatie wordt ingeslikt. Naarmate de buis door het maagdarmkanaal vordert, kan het slijmvlies van de slokdarm, maag en twaalfvingerige darm worden onderzocht.
De slokdarm van de meeste patiënten met symptomen van reflux ziet er normaal uit. Daarom zal endoscopie bij de meeste patiënten niet helpen bij de diagnose van GERD. Soms lijkt het slijmvlies van de slokdarm echter ontstoken (oesofagitis). Bovendien, als erosies (oppervlakkige breuken in de slokdarmwand) of zweren (diepere breuken in de voering) worden gezien, kan een diagnose van GERD vol vertrouwen worden gesteld. Endoscopie zal ook verschillende complicaties van GERD identificeren, met name zweren, stricturen en Barrett's slokdarm. Biopsieën kunnen ook worden verkregen.
Ten slotte kunnen andere veelvoorkomende problemen die GERD-achtige symptomen veroorzaken, worden gediagnosticeerd (bijvoorbeeld zweren, ontstekingen of kanker van de maag of twaalfvingerige darm) met EGD.
Biopsieën van de slokdarm die via de endoscoop worden verkregen, worden niet als erg nuttig beschouwd voor het diagnosticeren van GERD. Ze zijn echter nuttig bij het diagnosticeren van kankers of andere oorzaken van slokdarmontsteking dan zure reflux, met name infecties. Bovendien zijn biopsieën de enige manier om de cellulaire veranderingen van de Barrett-slokdarm te diagnosticeren. Meer recentelijk is gesuggereerd dat zelfs bij patiënten met GERD bij wie de slokdarm normaal lijkt voor het oog, biopsieën een verwijding van de ruimtes tussen de voeringcellen zullen laten zien, mogelijk een indicatie van schade. Het is echter te vroeg om te concluderen dat het zien van verbreding specifiek genoeg is om er zeker van te zijn dat GERD aanwezig is.
Vóór de introductie van endoscopie was een röntgenfoto van de slokdarm (een slokdarm genoemd) de enige manier om GERD te diagnosticeren. Patiënten slikten barium (contrastmateriaal) door en er werden röntgenfoto's gemaakt van de met barium gevulde slokdarm. Het probleem met de slokdarm was dat het een ongevoelige test was voor het diagnosticeren van GERD. Dat wil zeggen, het kon bij veel patiënten met GERD geen tekenen van GERD vinden omdat de patiënten weinig of geen schade hadden aan het slijmvlies van de slokdarm. De röntgenfoto's konden alleen de zeldzame complicaties van GERD laten zien, bijvoorbeeld zweren en stricturen. Röntgenfoto's zijn verlaten als een middel om GERD te diagnosticeren, hoewel ze nog steeds nuttig kunnen zijn samen met endoscopie bij de evaluatie van complicaties.
Wanneer GERD de keel of het strottenhoofd aantast en symptomen van hoest, heesheid of keelpijn veroorzaakt, bezoeken patiënten vaak een specialist in oor, neus en keel (KNO). De KNO-arts vindt vaak tekenen van ontsteking van de keel of strottenhoofd. Hoewel ziekten van de keel of het strottenhoofd meestal de oorzaak van de ontsteking zijn, kan GERD soms de oorzaak zijn. Dienovereenkomstig proberen KNO-specialisten vaak een zuuronderdrukkende behandeling om de diagnose GERD te bevestigen. Deze benadering heeft echter dezelfde problemen als hierboven besproken, die het gevolg zijn van het gebruik van de reactie op de behandeling om GERD te bevestigen.
Slokdarmzuurtests worden beschouwd als een "gouden standaard" voor het diagnosticeren van GERD. Zoals eerder besproken, is de reflux van zuur gebruikelijk in de algemene bevolking. Patiënten met de symptomen of complicaties van GERD hebben echter meer zuur terugvloeien dan personen zonder de symptomen of complicaties van GERD. Bovendien kunnen normale individuen en patiënten met GERD redelijk goed van elkaar worden onderscheiden door de hoeveelheid tijd dat de slokdarm zuur bevat.
De hoeveelheid tijd dat de slokdarm zuur bevat, wordt bepaald door een test die een 24-uurs slokdarm-pH-test wordt genoemd. (pH is een wiskundige manier om de hoeveelheid zuurgraad uit te drukken.) Voor deze test wordt een buisje (katheter) door de neus gevoerd en in de slokdarm geplaatst. Op de punt van de katheter bevindt zich een sensor die zuur detecteert. Het andere uiteinde van de katheter komt uit de neus, wikkelt zich terug over het oor en gaat naar de taille, waar het aan een recorder wordt bevestigd. Elke keer dat zuur terugvloeit in de slokdarm vanuit de maag, stimuleert het de sensor en registreert de recorder de episode van reflux. Na een periode van 20 tot 24 uur wordt de katheter verwijderd en wordt het record van reflux uit de recorder geanalyseerd.
Er zijn problemen met het gebruik van pH-testen voor het diagnosticeren van GERD. Ondanks dat normale individuen en patiënten met GERD op basis van pH-onderzoeken redelijk goed van elkaar te scheiden zijn, is de scheiding niet perfect. Daarom zullen sommige patiënten met GERD normale hoeveelheden zure reflux hebben en sommige patiënten zonder GERD zullen abnormale hoeveelheden zure reflux hebben. Het vereist iets anders dan de pH-test om de aanwezigheid van GERD te bevestigen, bijvoorbeeld typische symptomen, reactie op de behandeling of de aanwezigheid van complicaties van GERD. GERD kan ook met vertrouwen worden gediagnosticeerd wanneer episodes van brandend maagzuur correleren met zure reflux, zoals blijkt uit zuurtesten.
pH-testen hebben andere toepassingen bij het beheer van GERD dan alleen het diagnosticeren van GERD. De test kan bijvoorbeeld helpen bepalen waarom GERD-symptomen niet reageren op de behandeling. Misschien zal 10 tot 20 procent van de patiënten hun symptomen niet substantieel verbeteren door behandeling voor GERD. Dit gebrek aan respons op de behandeling kan worden veroorzaakt door een ineffectieve behandeling. Dit betekent dat het medicijn de productie van zuur door de maag niet voldoende onderdrukt en de zure terugvloeiing niet vermindert. Als alternatief kan het gebrek aan respons worden verklaard door een onjuiste diagnose van GERD. In beide situaties kan de pH-test erg handig zijn. Als uit testen blijkt dat er sprake is van substantiële terugvloeiing van zuur terwijl de medicatie wordt voortgezet, is de behandeling niet effectief en moet deze worden gewijzigd. Als testen een goede zuuronderdrukking aantoont met minimale terugvloeiing van zuur, is de diagnose GERD waarschijnlijk verkeerd en moeten andere oorzaken voor de symptomen worden gezocht.
pH-tests kunnen ook worden gebruikt om te beoordelen of reflux de oorzaak is van symptomen (meestal brandend maagzuur). Om deze evaluatie te maken, registreren patiënten tijdens de 24-uurs ph-test elke keer dat ze symptomen hebben. Vervolgens, wanneer de test wordt geanalyseerd, kan worden bepaald of zure reflux al dan niet optrad op het moment van de symptomen. Als reflux tegelijkertijd met de symptomen optrad, is reflux waarschijnlijk de oorzaak van de symptomen. Als er geen reflux was op het moment van symptomen, is het onwaarschijnlijk dat reflux de oorzaak van de symptomen is.
Ten slotte kunnen pH-tests worden gebruikt om patiënten te evalueren voorafgaand aan endoscopische of chirurgische behandeling voor GERD. Zoals hierboven besproken, zal ongeveer 20% van de patiënten een afname van hun symptomen hebben, ook al hebben ze geen GERD (het placebo-effect). Voorafgaand aan endoscopische of chirurgische behandeling is het belangrijk om deze patiënten te identificeren, omdat ze waarschijnlijk geen baat hebben bij de behandelingen. Het pH-onderzoek kan worden gebruikt om deze patiënten te identificeren, omdat ze normale hoeveelheden zure reflux zullen hebben.
A newer method for prolonged measurement (48 hours) of acid exposure in the esophagus utilizes a small, wireless capsule that is attached to the esophagus just above the LES. The capsule is passed to the lower esophagus by a tube inserted through either the mouth or the nose. After the capsule is attached to the esophagus, the tube is removed. The capsule measures the acid refluxing into the esophagus and transmits this information to a receiver that is worn at the waist. After the study, usually after 48 hours, the information from the receiver is downloaded into a computer and analyzed. The capsule falls off of the esophagus after 3-5 days and is passed in the stool. (The capsule is not reused.)
The advantage of the capsule over standard pH testing is that there is no discomfort from a catheter that passes through the throat and nose. Moreover, with the capsule, patients look normal (they don't have a catheter protruding from their noses) and are more likely to go about their daily activities, for example, go to work, without feeling self-conscious. Because the capsule records for a longer period than the catheter (48 versus 24 hours), more data on acid reflux and symptoms are obtained. Nevertheless, it is not clear whether obtaining additional information is important.
Capsule pH testing is expensive. Sometimes the capsule does not attach to the esophagus or falls off prematurely. For periods of time the receiver may not receive signals from the capsule, and some of the information about reflux of acid may be lost. Occasionally there is pain with swallowing after the capsule has been placed, and the capsule may need to be removed endoscopically. Use of the capsule is an exciting use of new technology although it has its own specific problems.
Esophageal motility testing determines how well the muscles of the esophagus are working. For motility testing, a thin tube (catheter) is passed through a nostril, down the back of the throat, and into the esophagus. On the part of the catheter that is inside the esophagus are sensors that sense pressure. A pressure is generated within the esophagus that is detected by the sensors on the catheter when the muscle of the esophagus contracts. The end of the catheter that protrudes from the nostril is attached to a recorder that records the pressure. During the test, the pressure at rest and the relaxation of the lower esophageal sphincter are evaluated. The patient then swallows sips of water to evaluate the contractions of the esophagus.
Esophageal motility testing has two important uses in evaluating GERD. The first is in evaluating symptoms that do not respond to treatment for GERD since the abnormal function of the esophageal muscle sometimes causes symptoms that resemble the symptoms of GERD. Motility testing can identify some of these abnormalities and lead to a diagnosis of an esophageal motility disorder. The second use is evaluation prior to surgical or endoscopic treatment for GERD. In this situation, the purpose is to identify patients who also have motility disorders of the esophageal muscle. The reason for this is that in patients with motility disorders, some surgeons will modify the type of surgery they perform for GERD.
Gastric emptying studies are studies that determine how well food empties from the stomach. As discussed above, about 20 % of patients with GERD have slow emptying of the stomach that may be contributing to the reflux of acid. For gastric emptying studies, the patient eats a meal that is labeled with a radioactive substance. A sensor that is similar to a Geiger counter is placed over the stomach to measure how quickly the radioactive substance in the meal empties from the stomach.
Information from the emptying study can be useful for managing patients with GERD. For example, if a patient with GERD continues to have symptoms despite treatment with the usual medications, doctors might prescribe other medications that speed-up emptying of the stomach. Alternatively, in conjunction with GERD surgery, they might do a surgical procedure that promotes a more rapid emptying of the stomach. Nevertheless, it is still debated whether a finding of reduced gastric emptying should prompt changes in the surgical treatment of GERD.
Symptoms of nausea, vomiting, and regurgitation may be due either to abnormal gastric emptying or GERD. An evaluation of gastric emptying, therefore, may be useful in identifying patients whose symptoms are due to abnormal emptying of the stomach rather than to GERD.
The acid perfusion (Bernstein) test is used to determine if chest pain is caused by acid reflux. For the acid perfusion test, a thin tube is passed through one nostril, down the back of the throat, and into the middle of the esophagus. A dilute, acid solution and a physiologic salt solution (similar to the fluid that bathes the body's cells) are alternately poured (perfused) through the catheter and into the esophagus. The patient is unaware of which solution is being infused. If the perfusion with acid provokes the patient's usual pain and perfusion of the salt solution produces no pain, it is likely that the patient's pain is caused by acid reflux.
The acid perfusion test, however, is used only rarely. A better test for correlating pain and acid reflux is a 24-hour esophageal pH or pH capsule study during which patients note when they are having pain. It then can be determined from the pH recording if there was an episode of acid reflux at the time of the pain. This is the preferable way of deciding if acid reflux is causing a patient's pain. It does not work well, however, for patients who have infrequent pain, for example every two to three days, which may be missed by a one or two day pH study. In these cases, an acid perfusion test may be reasonable.
One of the simplest treatments for GERD is referred to as life-style changes, a combination of several changes in habit, particularly related to eating.
As discussed above, reflux of acid is more injurious at night than during the day. At night, when individuals are lying down, it is easier for reflux to occur. The reason that it is easier is because gravity is not opposing the reflux, as it does in the upright position during the day. In addition, the lack of an effect of gravity allows the refluxed liquid to travel further up the esophagus and remain in the esophagus longer. These problems can be overcome partially by elevating the upper body in bed. The elevation is accomplished either by putting blocks under the bed's feet at the head of the bed or, more conveniently, by sleeping with the upper body on a foam rubber wedge. These maneuvers raise the esophagus above the stomach and partially restore the effects of gravity. It is important that the upper body and not just the head be elevated. Elevating only the head does not raise the esophagus and fails to restore the effects of gravity.
Elevation of the upper body at night generally is recommended for all patients with GERD. Nevertheless, most patients with GERD have reflux only during the day and elevation at night is of little benefit for them. It is not possible to know for certain which patients will benefit from elevation at night unless acid testing clearly demonstrates night reflux. However, patients who have heartburn, regurgitation, or other symptoms of GERD at night are probably experiencing reflux at night and definitely should elevate their upper body when sleeping. Reflux also occurs less frequently when patients lie on their left rather than their right sides.
Several changes in eating habits can be beneficial in treating GERD. Reflux is worse following meals. This probably is so because the stomach is distended with food at that time and transient relaxations of the lower esophageal sphincter are more frequent. Therefore, smaller and earlier evening meals may reduce the amount of reflux for two reasons. First, the smaller meal results in lesser distention of the stomach. Second, by bedtime, a smaller and earlier meal is more likely to have emptied from the stomach than is a larger one. As a result, reflux is less likely to occur when patients with GERD lie down to sleep.
Certain foods are known to reduce the pressure in the lower esophageal sphincter and thereby promote reflux. These foods should be avoided and include:
Fatty foods (which should be decreased) and smoking (which should be stopped) also reduce the pressure in the sphincter and promote reflux.
In addition, patients with GERD may find that other foods aggravate their symptoms. Examples are spicy or acid-containing foods, like citrus juices, carbonated beverages, and tomato juice. These foods should also be avoided if they provoke symptoms.
One novel approach to the treatment of GERD is chewing gum. Chewing gum stimulates the production of more bicarbonate-containing saliva and increases the rate of swallowing. After the saliva is swallowed, it neutralizes acid in the esophagus. In effect, chewing gum exaggerates one of the normal processes that neutralize acid in the esophagus. It is not clear, however, how effective chewing gum is in treating heartburn. Nevertheless, chewing gum after meals is certainly worth a try.
There is a variety of over-the-counter (for example, antacids and foam barriers) and prescription medications (for example, proton pump inhibitors, histamine antagonists, and promotility drugs) for treating GERD.
Despite the development of potent medications for the treatment of GERD, antacids remain a mainstay of treatment. Antacids neutralize the acid in the stomach so that there is no acid to reflux. The problem with antacids is that their action is brief. They are emptied from the empty stomach quickly, in less than an hour, and the acid then re-accumulates. The best way to take antacids, therefore, is approximately one hour after meals, which is just before the symptoms of reflux begin after a meal. Since the food from meals slows the emptying from the stomach, an antacid taken after a meal stays in the stomach longer and is effective longer. For the same reason, a second dose of antacids approximately two hours after a meal takes advantage of the continuing post-meal slower emptying of the stomach and replenishes the acid-neutralizing capacity within the stomach.
Antacids may be aluminum, magnesium, or calcium-based. Calcium-based antacids (usually calcium carbonate), unlike other antacids, stimulate the release of gastrin from the stomach and duodenum. Gastrin is the hormone that is primarily responsible for the stimulation of acid secretion by the stomach. Therefore, the secretion of acid rebounds after the direct acid-neutralizing effect of the calcium carbonate is exhausted. The rebound is due to the release of gastrin, which results in an overproduction of acid. Theoretically at least, this increased acid is not good for GERD.
Acid rebound, however, is not clinically important. That is, treatment with calcium carbonate is not less effective or safe than treatment with antacids not containing calcium carbonate. Nevertheless, the phenomenon of acid rebound is theoretically harmful. In practice, therefore, calcium-containing antacids such as Tums and Rolaids are not recommended for frequent use. The occasional use of these calcium carbonate-containing antacids, however, is not believed to be harmful. The advantages of calcium carbonate-containing antacids are their low cost, the calcium they add to the diet, and their convenience as compared to liquids.
Aluminum-containing antacids tend to cause constipation, while magnesium-containing antacids tend to cause diarrhea. If diarrhea or constipation becomes a problem, it may be necessary to switch antacids, or use antacids containing both aluminum and magnesium.
Although antacids can neutralize acid, they do so for only a short period. For substantial neutralization of acid throughout the day, antacids would need to be given frequently, at least every hour.
The first medication developed for the more effective and convenient treatment of acid-related diseases, including GERD, was a histamine antagonist, specifically cimetidine (Tagamet). Histamine is an important chemical because it stimulates acid production by the stomach. Released within the wall of the stomach, histamine attaches to receptors (binders) on the stomach's acid-producing cells and stimulates the cells to produce acid. Histamine antagonists work by blocking the receptor for histamine and thereby preventing histamine from stimulating the acid-producing cells. (Histamine antagonists are referred to as H2 antagonists because the specific receptor they block is the histamine type 2 receptor.)
As histamine is particularly important for the stimulation of acid after meals, H2 antagonists are best taken 30 minutes before meals. The reason for this timing is so that the H2 antagonists will be at peak levels in the body after the meal when the stomach is actively producing acid. H2 antagonists also can be taken at bedtime to suppress the nighttime production of acid.
H2 antagonists are very good for relieving the symptoms of GERD, particularly heartburn. However, they are not very good for healing the inflammation (esophagitis) that may accompany GERD. They are used primarily for the treatment of heartburn in GERD that is not associated with inflammation or complications, such as erosions or ulcers, strictures, or Barrett's esophagus.
Three different H2 antagonists are available by prescription, including cimetidine (Tagamet), nizatidine (Axid), and famotidine (Pepcid). Two of these, cimetidine (Tagamet HB) and famotidine (Pepcid AC, Zantac 360) are available over-the-counter (OTC), without the need for a prescription. However, the OTC dosages are lower than those available by prescription.
The second type of drug developed specifically for acid-related diseases, such as GERD, was a proton pump inhibitor (PPI), specifically, omeprazole (Prilosec). A PPI blocks the secretion of acid into the stomach by the acid-secreting cells. The advantage of a PPI over an H2 antagonist is that the PPI shuts off acid production more completely and for a longer period of time. Not only is the PPI good for treating the symptom of heartburn, but it also is good for protecting the esophagus from acid so that esophageal inflammation can heal.
PPIs are used when H2 antagonists do not relieve symptoms adequately or when complications of GERD such as erosions or ulcers, strictures, or Barrett's esophagus exist. Five different PPIs are approved for the treatment of GERD, including omeprazole (Prilosec, Dexilant), lansoprazole (Prevacid), rabeprazole (Aciphex), pantoprazole (Protonix), and esomeprazole (Nexium), and dexlansoprazole (Dexilant). A sixth PPI product consists of a combination of omeprazole and sodium bicarbonate (Zegerid). PPIs (except for Zegerid) are best taken an hour before meals. The reason for this timing is that the PPIs work best when the stomach is most actively producing acid, which occurs after meals. If the PPI is taken before the meal, it is at peak levels in the body after the meal when the acid is being made.
Pro-motility drugs work by stimulating the muscles of the gastrointestinal tract, including the esophagus, stomach, small intestine, and/or colon. One pro-motility drug, metoclopramide (Reglan), is approved for GERD. Pro-motility drugs increase the pressure in the lower esophageal sphincter and strengthen the contractions (peristalsis) of the esophagus. Both effects would be expected to reduce the reflux of acid. However, these effects on the sphincter and esophagus are small. Therefore, it is believed that the primary effect of metoclopramide may be to speed up emptying of the stomach, which also would be expected to reduce reflux.
Pro-motility drugs are most effective when taken 30 minutes before meals and again at bedtime. They are not very effective for treating either the symptoms or complications of GERD. Therefore, the pro-motility agents are reserved either for patients who do not respond to other treatments or are added to enhance other treatments for GERD.
Foam barriers provide a unique form of treatment for GERD. Foam barriers are tablets that are composed of an antacid and a foaming agent. As the tablet disintegrates and reaches the stomach, it turns into foam that floats on top of the liquid contents of the stomach. The foam forms a physical barrier to the reflux of liquid. At the same time, the antacid bound to the foam neutralizes acid that comes into contact with the foam. The tablets are best taken after meals (when the stomach is distended) and when lying down, both times when reflux is more likely to occur. Foam barriers are not often used as the first or only treatment for GERD. Rather, they are added to other drugs for GERD when the other drugs are not adequately effective in relieving symptoms. There is only one foam barrier, which is a combination of aluminum hydroxide gel, magnesium trisilicate, and alginate (Gaviscon).
The drugs described above usually are effective in treating the symptoms and complications of GERD. Nevertheless, sometimes they are not. For example, despite adequate suppression of acid and relief from heartburn, regurgitation, with its potential for complications in the lungs, may still occur. Moreover, the amounts and/or numbers of drugs that are required for satisfactory treatment are sometimes so great that drug treatment is unreasonable. In such situations, surgery can effectively stop reflux.
The surgical procedure that is done to prevent reflux is technically known as fundoplication and is called reflux surgery or anti-reflux surgery. During fundoplication, any hiatal hernial sac is pulled below the diaphragm and stitched there. In addition, the opening in the diaphragm through which the esophagus passes is tightened around the esophagus. Finally, the upper part of the stomach next to the opening of the esophagus into the stomach is wrapped around the lower esophagus to make an artificial lower esophageal sphincter. All of this surgery can be done through an incision in the abdomen (laparotomy) or using a technique called laparoscopy. During laparoscopy, a small viewing device and surgical instruments are passed through several small puncture sites in the abdomen. This procedure avoids the need for a major abdominal incision.
Surgery is very effective at relieving symptoms and treating the complications of GERD. Approximately 80% of patients will have good or excellent relief of their symptoms for at least 5 to 10 years. Nevertheless, many patients who have had surgery will continue to take drugs for reflux. It is not clear whether they take the drugs because they continue to have reflux and symptoms of reflux or if they take them for symptoms that are being caused by problems other than GERD. The most common complication of fundoplication is swallowed food that sticks at the artificial sphincter. Fortunately, the sticking usually is temporary. If it is not transient, endoscopic treatment to stretch (dilate) the artificial sphincter usually will relieve the problem. Only occasionally is it necessary to re-operate to revise the prior surgery.
Very recently, endoscopic techniques for the treatment of GERD have been developed and tested. One type of endoscopic treatment involves suturing (stitching) the area of the lower esophageal sphincter, which essentially tightens the sphincter.
A second type involves the application of radio-frequency waves to the lower part of the esophagus just above the sphincter. The waves cause damage to the tissue beneath the esophageal lining and a scar (fibrosis) forms. The scar shrinks and pulls on the surrounding tissue, thereby tightening the sphincter and the area above it.
A third type of endoscopic treatment involves the injection of materials into the esophageal wall in the area of the LES. The injected material is intended to increase pressure in the LES and thereby prevent reflux. In one treatment the injected material was a polymer. Unfortunately, the injection of polymer led to serious complications, and the material for injection is no longer available. Another treatment involving injection of expandable pellets also was discontinued. Limited information is available about a third type of injection which uses gelatinous polymethylmethacrylate microspheres.
Endoscopic treatment has the advantage of not requiring surgery. It can be performed without hospitalization. Experience with endoscopic techniques is limited. It is not clear how effective they are, especially long-term. Because the effectiveness and the full extent of potential complications of endoscopic techniques are not clear, it is felt generally that endoscopic treatment should only be done as part of experimental trials.
Transient LES relaxations appear to be the most common way in which acid reflux occurs. Although there is an available drug that prevents relaxations (baclofen), it has side effects that are too frequent to be generally useful. Much attention is being directed at the development of drugs that prevent these relaxations without accompanying side effects.
There are several ways to approach the evaluation and management of GERD. The approach depends primarily on the frequency and severity of symptoms, the adequacy of the response to treatment, and the presence of complications.
For infrequent heartburn, the most common symptom of GERD, life-style changes and an occasional antacid may be all that is necessary. If heartburn is frequent, daily non-prescription-strength (over-the-counter) H2 antagonists may be adequate. A foam barrier also can be used with the antacid or H2 antagonist.
If life-style changes and antacids, non-prescription H2 antagonists, and a foam barrier do not adequately relieve heartburn, it is time to see a physician for further evaluation and to consider prescription-strength drugs. The evaluation by the physician should include an assessment for possible complications of GERD based on the presence of such symptoms or findings as:
Clues to the presence of diseases that may mimic GERD, such as gastric or duodenal ulcers and esophageal motility disorders, should be sought.
If there are no symptoms or signs of complications and no suspicion of other diseases, a therapeutic trial of acid suppression with H2 antagonists often is used. If H2 antagonists are not adequately effective, a second trial, with the more potent PPIs, can be given. Sometimes, a trial of treatment begins with a PPI and skips the H2 antagonist. If treatment relieves the symptoms completely, no further evaluation may be necessary and the effective drug, the H2 antagonist or PPI, is continued. As discussed previously, however, there are potential problems with this commonly used approach, and some physicians would recommend a further evaluation for almost all patients they see.
If at the time of evaluation, there are symptoms or signs that suggest complicated GERD or a disease other than GERD or if the relief of symptoms with H2 antagonists or PPIs is not satisfactory, a further evaluation by endoscopy (EGD) definitely should be done.
There are several possible results of endoscopy and each requires a different approach to treatment. If the esophagus is normal and no other diseases are found, the goal of treatment simply is to relieve symptoms. Therefore, prescription strength H2 antagonists or PPIs are appropriate. If damage to the esophagus (esophagitis or ulceration) is found, the goal of treatment is healing the damage. In this case, PPIs are preferred over H2 antagonists because they are more effective for healing.
If complications of GERD, such as stricture or Barrett's esophagus are found, treatment with PPIs also is more appropriate. However, the adequacy of the PPI treatment probably should be evaluated with a 24-hour pH study during treatment with the PPI. (With PPIs, although the amount of acid reflux may be reduced enough to control symptoms, it may still be abnormally high. Therefore, judging the adequacy of suppression of acid reflux by only the response of symptoms to treatment is not satisfactory.) Strictures may also need to be treated by endoscopic dilatation (widening) of the esophageal narrowing. With Barrett's esophagus, periodic endoscopic examination should be done to identify pre-malignant changes in the esophagus.
If symptoms of GERD do not respond to maximum doses of PPI, there are two options for management. The first is to perform 24-hour pH testing to determine whether the PPI is ineffective or if a disease other than GERD is likely to be present. If the PPI is ineffective, a higher dose of PPI may be tried. The second option is to go ahead without 24 hour pH testing and to increase the dose of PPI. Another alternative is to add another drug to the PPI that works in a way that is different from the PPI, for example, a pro-motility drug or a foam barrier. If necessary, all three types of drugs can be used. If there is not a satisfactory response to this maximal treatment, 24 hour pH testing should be done.
Who should consider surgery or, perhaps, an endoscopic treatment trial for GERD? (As mentioned previously, the effectiveness of the recently developed endoscopic treatments remains to be determined.) Patients should consider surgery if they have regurgitation that cannot be controlled with drugs. This recommendation is particularly important if the regurgitation results in infections in the lungs or occurs at night when aspiration into the lungs is more likely. Patients also should consider surgery if they require large doses of PPI or multiple drugs to control their reflux. It is debated whether or not a desire to be free of the need to take life-long drugs to prevent symptoms of GERD is by itself a satisfactory reason for having surgery.
Some physicians - primarily surgeons - recommend that all patients with Barrett's esophagus should have surgery. This recommendation is based on the belief that surgery is more effective than endoscopic surveillance or ablation of the abnormal tissue followed by treatment with acid-suppressing drugs in preventing both the reflux and the cancerous changes in the esophagus. There are no studies, however, demonstrating the superiority of surgery over drugs or ablation for the treatment of GERD and its complications. Moreover, the effectiveness of drug treatment can be monitored with 24 hour pH testing.
One unresolved issue in GERD is the inconsistent relationships among acid reflux, heartburn, and damage to the lining of the esophagus (esophagitis and the complications).
Clearly, we have much to learn about the relationship between acid reflux and esophageal damage, and about the processes (mechanisms) responsible for heartburn. This issue is of more than passing interest. Knowledge of the mechanisms that produce heartburn and esophageal damage raises the possibility of new treatments that would target processes other than acid reflux.
One of the more interesting theories that has been proposed to answer some of these questions involves the reason for pain when acid refluxes. It often is assumed that the pain is caused by irritating acid contacting an inflamed esophageal lining. But the esophageal lining usually is not inflamed. It is possible therefore, that the acid is stimulating the pain nerves within the esophageal wall just beneath the lining. Although this may be the case, a second explanation is supported by the work of one group of scientists. These scientists find that heartburn provoked by acid in the esophagus is associated with contraction of the muscle in the lower esophagus. Perhaps it is the contraction of the muscle that somehow leads to the pain. It also is possible, however, that the contraction is an epiphenomenon, that is, refluxed acid stimulates pain nerves and causes the muscle to contract, but it is not the contraction that causes the pain. More studies will be necessary before the exact mechanism(s) that causes heartburn is clear.
There are potentially injurious agents that can be refluxed other than acid, for example, bile. Until recently it has been impossible or difficult to accurately identify non-acid reflux and, therefore, to study whether or not non-acid reflux is injurious or can cause symptoms.
A new technology allows the accurate determination of non-acid reflux. This technology uses the measurement of impedance changes within the esophagus to identify reflux of liquid, be it acid or non-acid. By combining measurement of impedance and pH it is possible to identify reflux and to tell if the reflux is acid or non-acid. It is too early to know how important non-acid reflux is in causing esophageal damage, symptoms, or complications, but there is little doubt that this new technology will be able to resolve the issues surrounding non-acid reflux.
 De 7 dodelijkste algemene spoedoperaties
Laatste preventie- en welzijnsnieuws Het aantal doden door koolmonoxide stijgt tijdens stroomuitval Rode Kruis zegt bloedtoevoer gevaarlijk laag Een frisse start met wat je ook doet in 22 Er zijn gee
De 7 dodelijkste algemene spoedoperaties
Laatste preventie- en welzijnsnieuws Het aantal doden door koolmonoxide stijgt tijdens stroomuitval Rode Kruis zegt bloedtoevoer gevaarlijk laag Een frisse start met wat je ook doet in 22 Er zijn gee
 Cystinurie - Nierstenen
De stenen die hier in grootte worden vergeleken met een kwart (een munt van US $ 0,25) kwamen van de nier van een jonge vrouw met cystinurie, het meest voorkomende defect dat bekend is bij het transpo
Cystinurie - Nierstenen
De stenen die hier in grootte worden vergeleken met een kwart (een munt van US $ 0,25) kwamen van de nier van een jonge vrouw met cystinurie, het meest voorkomende defect dat bekend is bij het transpo
 Spinnenbeten (Black Widow en Brown Recluse) Symptomen
Wat moet je weten over spinnenbeten? Fotos Black Widow-spin en bruine kluizenaarspin De meeste spinnen in de VS zijn ongevaarlijk. De beten van zwarte weduwen en bruine kluizenaars zijn echter gev
Spinnenbeten (Black Widow en Brown Recluse) Symptomen
Wat moet je weten over spinnenbeten? Fotos Black Widow-spin en bruine kluizenaarspin De meeste spinnen in de VS zijn ongevaarlijk. De beten van zwarte weduwen en bruine kluizenaars zijn echter gev