 Čo je HCV, ako sa prenáša, existujú príznaky a je liečiteľná?
Čo je HCV, ako sa prenáša, existujú príznaky a je liečiteľná?Väčšina ľudí, ktorí sa nakazia hepatitídou C (hepatitídou C), nemá žiadne príznaky. Avšak tí, ktorí majú príznaky, môžu zažiť:
Infekcia vírusom hepatitídy C je infekcia pečene spôsobená vírusom hepatitídy C (tiež označovaný ako HCV alebo hepatitída C). Pre ľudský imunitný systém je ťažké odstrániť hepatitídu C z tela a infekcia hepatitídou C sa zvyčajne stáva chronickou. V priebehu desaťročí chronická infekcia hepatitídou C poškodzuje pečeň a môže spôsobiť zlyhanie pečene. V USA CDC odhaduje, že v roku 2016 sa vyskytlo približne 41 200 nových prípadov hepatitídy C. Keď vírus prvýkrát vstúpi do tela, zvyčajne sa nevyskytujú žiadne príznaky, takže toto číslo je odhad. Približne 75 % – 85 % novoinfikovaných ľudí sa stane chronicky infikovanými. Odhaduje sa, že v USA je viac ako 2 milióny ľudí chronicky infikovaných hepatitídou C. Infekcia sa najčastejšie zisťuje medzi ľuďmi vo veku 40 až 60 rokov, čo odzrkadľuje vysokú mieru infekcie v 70. a 80. rokoch 20. storočia. V Spojených štátoch každoročne zomrie 8 000 až 10 000 úmrtí súvisiacich s infekciou hepatitídou C. Infekcia HCV je hlavnou príčinou transplantácie pečene v USA a je rizikovým faktorom rakoviny pečene. V roku 2016 18 153 úmrtných listov uvádzalo HCV ako prispievajúcu príčinu smrti; toto sa považuje za podhodnotené.
Asi u 10 % až 20 % tých, u ktorých sa vyvinie chronická HCV, sa v priebehu 20 až 30 rokov vyvinie cirhóza. Progresiu do cirhózy môže urýchliť vek nad 50 rokov, mužské pohlavie, konzumácia alkoholu, nealkoholické stukovatenie pečene (NASH), koinfekcia hepatitídou B alebo HIV a lieky potláčajúce imunitu. Infekcia HCV je hlavnou príčinou transplantácie pečene v dôsledku zlyhania pečene v USA
Tí, ktorí majú cirhózu spôsobenú HCV, majú tiež ročné riziko rakoviny pečene (hepatóm alebo hepatocelulárny karcinóm) približne 1%-5%.
Hepatitída znamená zápal pečene. Hepatitída C je jedným z niekoľkých vírusov, ktoré môžu spôsobiť vírusovú hepatitídu. Nesúvisí s inými bežnými vírusmi hepatitídy (napríklad hepatitída A alebo hepatitída B). Hepatitída C je členom Flaviviridae rodina vírusov. Medzi ďalších členov tejto rodiny vírusov patria tie, ktoré spôsobujú žltú zimnicu a horúčku dengue.
Existuje najmenej šesť rôznych genotypov (kmeňov) vírusu, ktoré majú rôzne genetické profily (genotypy 1 až 6). V USA je genotyp 1 najbežnejším kmeňom hepatitídy C. Dokonca aj v rámci jedného genotypu môžu existovať určité variácie (napríklad genotyp 1a a 1b). Genotypizácia sa používa na usmernenie liečby, pretože niektoré vírusové genotypy reagujú na niektoré terapie lepšie ako na iné.
Podobne ako vírus ľudskej imunodeficiencie (HIV), aj hepatitída C sa veľmi rýchlo množí a dosahuje v tele veľmi vysoké hladiny. Gény, ktoré tvoria povrchové proteíny vírusu, tiež rýchlo mutujú (menia sa) a denne vznikajú tisíce genetických variácií vírusu („kvázidruhov“). Pre telo je nemožné držať krok s tvorbou anti-HCV protilátok proti všetkým kvázi druhom cirkulujúcim naraz. Zatiaľ nebolo možné vyvinúť účinnú vakcínu, pretože vakcína musí chrániť pred všetkými genotypmi.
Infekcia hepatitídou C v pečeni spúšťa imunitný systém, čo vedie k zápalu. Asi 20 % až 30 % akútne infikovaných bude pociťovať typické symptómy hepatitídy, ako je bolesť brucha, žltačka, tmavý moč alebo hlinená stolica. Chronická hepatitída C však zvyčajne nespôsobuje žiadne príznaky až do veľmi neskorého štádia choroby a hepatitídu C chorí označujú ako „spiaci drak“. V priebehu niekoľkých rokov alebo desaťročí môže chronický zápal spôsobiť smrť pečeňových buniek a zjazvenie ("fibrózu"). Rozsiahle zjazvenie v pečeni sa nazýva cirhóza. To postupne zhoršuje vitálne funkcie pečene. Cirhotická pečeň je náchylnejšia na rakovinu pečene. Pitie alkoholu urýchľuje poškodenie pečene hepatitídou C. Súčasná infekcia HIV, ako aj akútna infekcia hepatitídou A alebo B tiež urýchli progresiu do cirhózy.
Asi 70 % až 80 % ľudí nemá žiadne príznaky, keď prvýkrát dostanú infekciu HCV. Zvyšných 20 % - 30 % môže mať
Skoré príznaky hepatitídy C môžu zahŕňať tmavý moč, žlté oči alebo hlinenú stolicu, hoci je to nezvyčajné. V priebehu času sa u ľudí s chronickou infekciou HCV môžu vyvinúť príznaky zápalu pečene, ktoré naznačujú, že infekcia môže byť prítomná. Infikovaní jedinci sa môžu ľahko unaviť alebo sa môžu sťažovať na nešpecifické symptómy. Neskoršie príznaky a príznaky cirhózy často chýbajú, kým zápal nie je dostatočne pokročilý. S progresiou cirhózy sa symptómy a príznaky zvyšujú a môžu zahŕňať:
Pretože hepatitída C sa prenáša vystavením krvi, neexistuje žiadne špecifické obdobie nákazlivosti. Ľudia, u ktorých sa rozvinie chronická hepatitída C, nesú vírus v krvi, a preto sú nákazliví pre ostatných po celý život, pokiaľ sa z hepatitídy C nevyliečia.
Je ťažké s istotou povedať, aká je inkubačná doba pre hepatitídu C, pretože väčšina ľudí, ktorí sú infikovaní hepatitídou C, nemá príznaky v ranom štádiu infekcie. U tých, u ktorých sa objavia príznaky skoro po infikovaní (v priemere 2 až 12 týždňov, ale môže to byť aj dlhšie), sa vyskytnú mierne gastrointestinálne príznaky, ktoré nemusia viesť k návšteve lekára.
Väčšina príznakov a symptómov infekcie hepatitídy C sa týka pečene. Menej často môže infekcia hepatitídou C postihnúť aj iné orgány ako pečeň.
Infekcia hepatitídy C môže spôsobiť, že telo produkuje abnormálne protilátky nazývané kryoglobulíny. Kryoglobulíny spôsobujú zápal tepien (vaskulitídu). To môže poškodiť kožu, kĺby a obličky. Pacienti s kryoglobulinémiou (kryoglobulíny v krvi) môžu mať
Okrem toho sa u infikovaných jedincov s kryoglobulinémiou môže vyvinúť Raynaudov fenomén, pri ktorom sa sfarbia prsty na rukách a nohách (biele, potom fialové, potom červené) a pri nízkych teplotách sú bolestivé.
Pracovná skupina preventívnych zdravotníckych služieb v USA odporúča, aby všetci dospelí narodení v rokoch 1945 až 1965 boli raz rutinne testovaní na hepatitídu C, bez ohľadu na to, či sú prítomné rizikové faktory pre hepatitídu C. Jednorazové testovanie sa odporúča aj pre:
Ľudia, ktorí mohli byť vystavení hepatitíde C v predchádzajúcich 6 mesiacoch, by mali byť testovaní na vírusovú RNA záťaž namiesto anti-HCV protilátky, pretože protilátka nemusí byť prítomná až 12 týždňov alebo dlhšie po infekcii, hoci HCV RNA môže byť detekovateľná v krvi už 2-3 týždne po infekcii.
Vo všeobecnosti môže byť ročný skríning vhodný pre ľudí s pretrvávajúcimi rizikovými faktormi, ako sú opakované sexuálne prenosné choroby (STD) alebo mnohí sexuálni partneri, pokračujúce užívanie IV drog alebo dlhodobých sexuálnych partnerov ľudí s hepatitídou C. Či testovať alebo nie títo ľudia sa určujú na základe rozhodnutia od prípadu k prípadu.
Pri každom tehotenstve existuje 4-7% riziko prenosu HCV z matky na dieťa. V súčasnosti neexistuje odporúčanie CDC pre rutinný skríning hepatitídy C počas tehotenstva a v súčasnosti neexistuje odporúčaný liek na zabránenie prenosu z matky na dieťa (profylaxia). CDC však monitoruje výsledky výskumu a v budúcnosti môže vydať odporúčania, keď sa objavia dôkazy.
Zatiaľ čo údaje sú stále obmedzené, nedávna štúdia s viac ako 1 000 prípadmi v Spojenom kráľovstve zistila, že 11 % dojčiat bolo infikovaných pri narodení a že u týchto dojčiat sa pravdepodobne rozvinie cirhóza v ranom veku 30 rokov. Prípad pre skríning HCV počas tehotenstva zahŕňa potenciál bezpečne liečiť matky počas tehotenstva priamo pôsobiacimi antivírusovými látkami (DAA) na liečbu matky pred rozvojom cirhózy, prevenciu prenosu dojčiat a prevenciu prenosu na iné osoby. Deťom narodeným matkám infikovaným HCV možno tiež ponúknuť liečbu v ranom veku na prevenciu cirhózy, ako aj prenosu na iných. Na dosiahnutie týchto cieľov bude dôležitá koordinácia starostlivosti medzi viacerými odborníkmi.
Deti matiek infikovaných HCV môžu byť vyšetrené na hepatitídu C už vo veku 1-2 mesiacov pomocou testovania vírusovej záťaže hepatitídy C alebo PCR (pozri Krvné testy na hepatitídu C). Protilátky proti hepatitíde C prenesené z matky na dieťa budú prítomné až 18 mesiacov, takže deti by mali byť testované na HCV protilátky najskôr.
Hepatitídu C lieči buď gastroenterológ, hepatológ (gastroenterológ s dodatočným vzdelaním v oblasti ochorenia pečene) alebo špecialista na infekčné choroby. Liečebný tím môže zahŕňať viac ako jedného špecialistu v závislosti od rozsahu poškodenia pečene. Chirurgovia, ktorí sa špecializujú na chirurgiu pečene vrátane transplantácie pečene, sú súčasťou lekárskeho tímu a mali by vidieť pacientov s pokročilým ochorením (zlyhanie pečene alebo cirhóza) skôr, ako pacient potrebuje transplantáciu pečene. Môžu byť schopní identifikovať problémy, ktoré je potrebné riešiť pred zvážením operácie. Medzi ďalšie osoby, ktoré môžu byť nápomocné pri liečbe pacientov, patria dietológovia, ktorí konzultujú otázky výživy, a lekárnici, ktorí pomáhajú pri liečbe liekov.
Na diagnostiku infekcie hepatitídou C existuje niekoľko krvných testov. Krv môže byť testovaná na protilátky proti hepatitíde C (anti-HCV protilátka). Vytvorenie protilátok po počiatočnej infekcii hepatitídou C trvá v priemere asi 8 – 12 týždňov a až 6 mesiacov, takže skríning protilátok môže vynechať niekoľko novoinfikovaných jedincov. Mať protilátky nie je absolútnou indikáciou aktívneho, množiaceho sa vírusu hepatitídy C, ale ak je test na protilátky pozitívny (protilátka je prítomná), štatistická pravdepodobnosť aktívnej infekcie je vyššia ako 99 %.
Na meranie množstva vírusu hepatitídy C v krvi človeka je k dispozícii niekoľko testov (vírusová záťaž). RNA vírusu hepatitídy C možno identifikovať pomocou typu testu nazývaného polymerázová reťazová reakcia (PCR), ktorý deteguje cirkulujúci vírus v krvi už 2-3 týždne po infekcii, takže sa môže použiť na detekciu podozrenia na akútnu infekciu hepatitídou C skorá infekcia. Používa sa tiež na určenie, či je aktívna hepatitída prítomná u niekoho, kto má protilátky proti hepatitíde C, a na sledovanie vírusovej záťaže počas liečby.
Vykonávajú sa aj krvné testy na identifikáciu genotypov HCV. Genotypy reagujú rôzne na rôznu liečbu, takže táto informácia je dôležitá pri výbere najvhodnejšieho liečebného režimu.
Odhad fibrózy pečene pomocou krvných testov je tiež celkom spoľahlivý pri diagnostikovaní klinicky významných jaziev; tieto zahŕňajú FIB-4, FibroSure, Fibrotest a index pomeru aspartátaminotransferázy k trombocytom (APRI).
Ďalším krokom je určenie úrovne zjazvenia pečene, ktoré sa vyskytlo. Biopsia pečene umožňuje vyšetrenie malej vzorky pečeňového tkaniva pod mikroskopom, avšak biopsia pečene je invazívny test a má významné riziko krvácania. Môže tiež vynechať abnormálne oblasti v ranom štádiu ochorenia.
Neinvazívne testy vo veľkej miere nahradili biopsiu pečene, s výnimkou špeciálnych situácií. Stuhnutosť pečene naznačuje, že môže byť prítomné pokročilé zjazvenie pečene alebo cirhóza pečene. Transient elastography may be used to measure this stiffness by ultrasound or magnetic resonance imaging (MRI).
Pre-treatment evaluation for hepatitis C also should include:
Interferons, for example, Roferon-A and Infergen, and pegylated interferons such as Peg-Intron T , Pegasys, were mainstays of treatment for years. Interferons produced sustained viral response (SVR, or cure) of up to 15%. Later, peglatedll forms produced SVR of 50%-80%. These drugs were injected, had many adverse effects, required frequent monitoring, and were often combined with oral ribavirin, which caused anemia. Treatment durations ranged up to 48 weeks.
Direct-acting anti-viral agents (DAAs) are antiviral drugs that act directly on hepatitis C multiplication.
Hepatitis C treatment is best discussed with a doctor or specialist familiar with current and developing options as this field is changing, and even major guidelines may become outdated quickly.
The latest treatment guidelines by the American Association for the Study of Liver Disease (AASLD) and Infectious Disease Society of America (IDSA) recommends use of DAAs as first-line treatment for hepatitis C infection. The choice of DAA varies by specific virus genotype, and the presence or absence of cirrhosis. In the U.S., specific insurance providers also might influence the choice due to the high cost of DAAs. Although the individual, public health, and cost benefits of treating all patients with hepatitis C is clear, the most difficult barrier to treating all people with HCV is the very high cost of the drug regimens. Patients are encouraged to discuss options with their health care professional.
Treatment is recommended in all patients with chronic hepatitis C unless they have a short life expectancy that is not related to liver disease. Severe life-threatening liver disease may require liver transplantation. Newer therapies with DAAs have allowed more and more patients to be treated.
The ultimate goals of antiviral therapy are to
A side goal is preventing co-infections with other hepatitis viruses, such as A and B, which can cause more liver disease than HCV alone. These can be prevented by vaccines and treatment.
When people first get hepatitis C, the infection is said to be acute. Most people with acute hepatitis C do not have symptoms so they are not recognized as being infected. However, some have low-grade fever, fatigue or other symptoms that lead to an early diagnosis. Others who become infected and have a known exposure to an infected source, such as a needlestick injury, are monitored closely.
Treatment decisions should be made on a case-by-case basis. Response to treatment is higher in acute hepatitis infection than chronic infection. However, many experts prefer to hold off treatment for 8-12 weeks to see whether the patient naturally eliminates the virus without treatment. Approaches to treatment are evolving. Patients with acute hepatitis C infection should discuss treatment options with a health care professional who is experienced in treating the disease. There is no established treatment regimen at this time.
If the hepatitis C RNA remains undetectable at the end of the treatment and follow-up period, this is called a sustained virologic response (SVR) and is considered a cure. Over 90% of people treated with DAAs are cured. These people have significantly reduced liver inflammation, and liver scarring may even be reversed.
About 5% of people who are treated for HCV infection are not cured by some of the older regimens. These people may still have options for cure with the newer regimens.
Few people with hepatitis C are at risk for problems if they are treated, however there are some factors that affect treatment regimens, such as concurrent HIV medications and kidney dysfunction. Some drugs are not safe for people with cirrhosis. Individuals who are unable to comply with the treatment schedule for psychological reasons or ongoing drug or alcohol abuse may not be good candidates for treatment because the drugs are very costly and require adherence to the pill regimen and regular follow-up visits. There are some important drug interactions with some of the medications that should be considered by the health care professional.
People with past hepatitis B or who have chronic active hepatitis B should not be treated for HCV without treating for HBV as well. As highly effective treatment for HCV has emerged, reports of serious hepatitis B have come to light. Similar to HCV, hepatitis B usually does not clear from the liver after acute infection, even though it is far less likely to cause chronic active hepatitis than hepatitis C infection. It remains dormant in most people, but it can reactivate with changes in the immune system. It is not clear why eliminating the HCV can allow the HBV infection to flare up. Hepatitis B screening is an important part of the hepatitis C evaluation. Those who have laboratory evidence of active or past infection with HBV should be monitored while receiving HCV treatment.
Compared to interferons and ribavirin drugs, the side effects of DAAs are far fewer and more tolerable. These side effects usually do not require discontinuation of therapy and are self-limiting after completion of therapy.
Patients with hepatitis B co-infection should be monitored for symptoms of reactivation of hepatitis, which are the same as the symptoms of acute hepatitis. The treating doctor may perform blood screening for this as well.
Hepatitis C is the leading reason for 40% to 45% of liver transplants in the U.S. Hepatitis C usually recurs after transplantation and infects the new liver. Approximately 25% of these patients with recurrent hepatitis will develop cirrhosis within five years of transplantation. Despite this, the five-year survival rate for patients with hepatitis C is similar to that of patients who are transplanted for other types of liver disease.
Most transplant centers delay therapy until recurrent hepatitis C in the transplanted liver is confirmed. Oral, highly effective, direct-acting antivirals have shown encouraging results in patients who have undergone liver transplantation for hepatitis C infection and have recurrent hepatitis C. The choice of therapy needs to be individualized and is rapidly evolving.
Once patients successfully complete treatment, the viral load after treatment determines if there is an SVR or cure. If cure is achieved (undetectable viral load after treatment), no further additional testing is recommended unless the patient has cirrhosis. Those who are not cured will need continued monitoring for progression of liver disease and its complications.
While cure eliminates worsening of fibrosis by hepatitis C, complications may still affect those with cirrhosis. These individuals still need regular screening for liver cancer as well as monitoring for esophageal varices that may bleed.
Because hepatitis B co-infection may reactivate or worsen even after treatment for HCV, monitoring for hepatitis symptoms may be needed after the end of therapy.
At this time there are no effective home or over-the-counter treatments for hepatitis C.
Over several years or decades, chronic inflammation may cause death of liver cells and cirrhosis (scaring, fibrosis). When the liver becomes cirrhotic, it becomes stiff, and it cannot perform its normal functions of clearing waste products from the blood. As fibrosis worsens, symptoms of liver failure begin to appear. This is called "decompensated cirrhosis " or "end-stage liver disease. " Symptoms of end-stage liver disease include:
The liver and spleen have an important function of clearing bacteria from the blood stream. Cirrhosis affects many areas of immune function, including attraction of white blood cells to bacteria, reduced killing of bacteria, reduced production of proteins involved in immune defenses, and decreased life span of white blood cells involved in immune defenses. This may be referred to as having cirrhosis-associated immune dysfunction syndrome or CAIDS.
Transmission of hepatitis C can be prevented in several ways.
Prevention programs aim at needle sharing among drug addicts. Needle exchange programs and education have reduced transmission of hepatitis C infection. However, IV drug users are a difficult to reach population, and rates of hepatitis C remain high among them.
Among health care workers, safe needle-usage techniques have been developed to reduce accidental needlesticks. Newer needle systems prevent manual recapping of needles after use of syringes, which is a frequent cause of accidental needlesticks
There is no clear way to prevent hepatitis C transmission from mother to fetus at this time.
People with multiple sexual partners should use barrier precautions such as condoms to limit the risk of hepatitis C and other sexually transmitted diseases, including HIV.
If one partner is infected, monogamous couples may want to consider the low risk of transmission of hepatitis C infection when deciding whether to use condoms during sex. Some couples may decide to use them and some may not.
Screening of the blood supply has almost eliminated the risk of transmission of hepatitis C infection through transfusion.
People with hepatitis C infection should not share razors or toothbrushes with others because of the possibility that these items may be contaminated with blood.
People who want to get a body piercing(s) or tattoo(s) are encouraged to do so only at licensed piercing and tattoo shops (facilities), and verify that the body piercing or tattoo shop uses infection-control practices.
It is critical that physicians and clinics follow manufacturers and regulatory agency directions for sterilizing/cleaning instruments and that disposable instruments be discarded properly. There is no need to use special isolation procedures when dealing with hepatitis C infected patients.
In general, among patients with untreated hepatitis C:
Drinking alcohol and acquiring other hepatitis viruses are risk factors for worse liver disease. People with chronic hepatitis C should avoid drinking alcohol and should be screened for antibodies to hepatitis A and B. If they do not have antibodies, they should be vaccinated against these other hepatitis viruses.
People with hepatitis C should be educated about preventing HIV infection. Infection with both HIV and hepatitis C speeds up and worsens liver damage caused by hepatitis C. Hepatitis C also can affect the HIV infection and how it is treated. About 25% of people with HIV infection are co-infected (also infected) with hepatitis C, and up to 90% of IV drug users with HIV are co-infected with hepatitis C. Screening for hepatitis viruses is important in all people infected with HIV, just as screening for HIV is important in people who have hepatitis C.
Liver cancer (hepatocellular carcinoma, or hepatoma) is associated with cirrhosis from chronic hepatitis C. Some experts recommend screening patients with hepatitis C infection and cirrhosis for liver cancer periodically.
As our knowledge of hepatitis C increases, more and more patients are being diagnosed with chronic infection. Current research is very active and includes diagnosis, natural history, treatment, and vaccine development. Thus the field is constantly changing, with new guidelines added frequently.
 Hepatitída (vírusová hepatitída A, B, C, D, E, G)
Hepatitída (vírusová hepatitída A, B, C, D, E, G)
 Ako nájsť hlavnú príčinu vašich tráviacich problémov
Ako nájsť hlavnú príčinu vašich tráviacich problémov
 Schválené Xermelo pre hnačku súvisiacu s nádorom
Schválené Xermelo pre hnačku súvisiacu s nádorom
 Zbavte sa bolestí krku a hornej časti chrbta raz a navždy
Zbavte sa bolestí krku a hornej časti chrbta raz a navždy
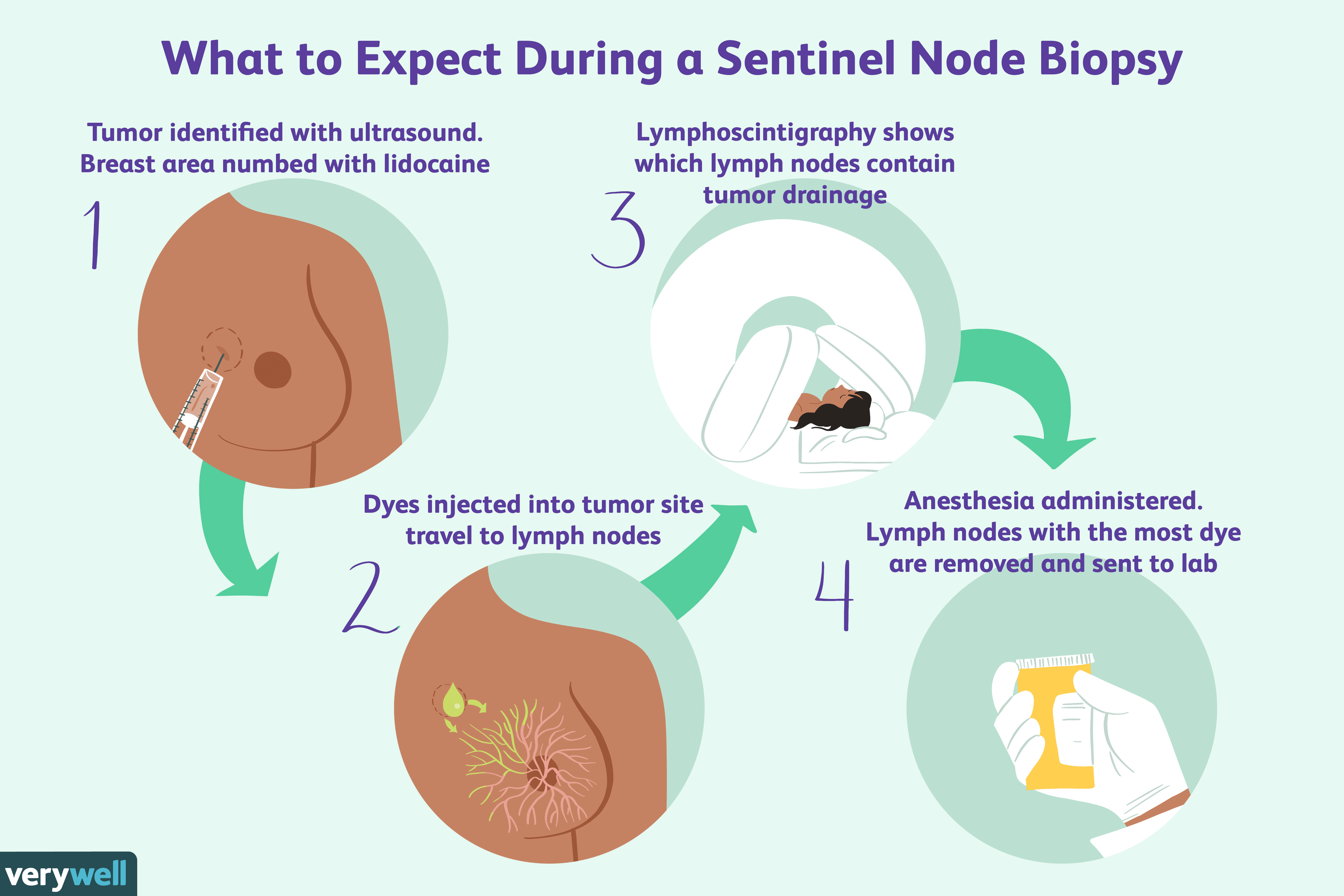 Prehľad rakoviny prsníka s pozitívnymi lymfatickými uzlinami
Prehľad rakoviny prsníka s pozitívnymi lymfatickými uzlinami
 Čo je laparoskopická kolektómia ľavej strany/hemikolektómia?
Čo je laparoskopická kolektómia ľavej strany/hemikolektómia?
 Čo je SIBO?
Čo presne je prerastanie baktérií v tenkom čreve? Zjednodušene povedané, prerastanie baktérií v tenkom čreve (SIBO) je premnoženie normálnych baktérií v tenkom čreve. Nie sú to patogénne baktérie, al
Čo je SIBO?
Čo presne je prerastanie baktérií v tenkom čreve? Zjednodušene povedané, prerastanie baktérií v tenkom čreve (SIBO) je premnoženie normálnych baktérií v tenkom čreve. Nie sú to patogénne baktérie, al
 Hlavné body a kľúčové informácie zo stretnutia Boston Bacterial Meeting (BBM) v roku 2019
Boston Bacterial Meeting (BBM) je výročná konferencia, na ktorej sa stretávajú odborníci na bakteriológiu z oblasti Bostonu a z celého sveta. Je 25 th iterácia prebehla medzi 6. júnom th a 7. júna
Hlavné body a kľúčové informácie zo stretnutia Boston Bacterial Meeting (BBM) v roku 2019
Boston Bacterial Meeting (BBM) je výročná konferencia, na ktorej sa stretávajú odborníci na bakteriológiu z oblasti Bostonu a z celého sveta. Je 25 th iterácia prebehla medzi 6. júnom th a 7. júna
 Zobrazovanie magnetickou rezonanciou (MRI sken)
Definícia a fakty skenovania magnetickou rezonanciou (MRI) Obrázok:Zdravotnícky technik pripravuje pacienta na magnetickú rezonanciu na kontrolu možného nádoru mozgu Zobrazovanie magnetickou rezonanc
Zobrazovanie magnetickou rezonanciou (MRI sken)
Definícia a fakty skenovania magnetickou rezonanciou (MRI) Obrázok:Zdravotnícky technik pripravuje pacienta na magnetickú rezonanciu na kontrolu možného nádoru mozgu Zobrazovanie magnetickou rezonanc