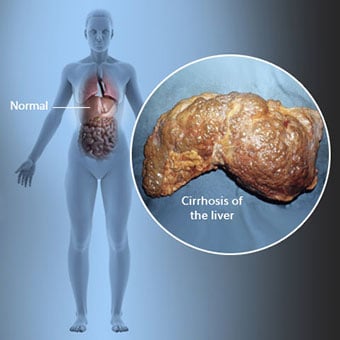
 Cirozė yra kepenų ligos komplikacija, kuri apima kepenų ląstelių praradimą ir negrįžtamą kepenų randėjimą.
Cirozė yra kepenų ligos komplikacija, kuri apima kepenų ląstelių praradimą ir negrįžtamą kepenų randėjimą. Asmenys, sergantys ciroze, gali turėti nedaug arba visai nejausti kepenų ligos simptomų ir požymių. Kai kurie simptomai gali būti nespecifiniai, tai yra, jie nereiškia, kad jų priežastis yra kepenys. Kai kurie dažniausiai pasitaikantys cirozės simptomai ir požymiai:
Asmenims, sergantiems ciroze, taip pat atsiranda simptomų ir požymių dėl cirozės komplikacijų.
 Yra daug cirozės priežasčių, įskaitant chemines medžiagas (pvz., alkoholį, riebalus ir tam tikrus vaistus), virusus, toksines medžiagas. metalų ir autoimuninės kepenų ligos, kai organizmo imuninė sistema atakuoja kepenis.
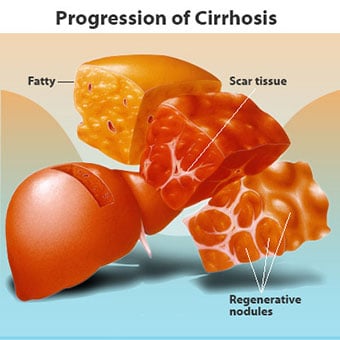
Yra daug cirozės priežasčių, įskaitant chemines medžiagas (pvz., alkoholį, riebalus ir tam tikrus vaistus), virusus, toksines medžiagas. metalų ir autoimuninės kepenų ligos, kai organizmo imuninė sistema atakuoja kepenis. Cirozė yra daugelio kepenų ligų, kurioms būdinga nenormali kepenų struktūra ir funkcija, komplikacija. Ligos, sukeliančios cirozę, tai daro todėl, kad jos pažeidžia ir žudo kepenų ląsteles, o po to uždegimas ir atstatymas, susijęs su mirštančiomis kepenų ląstelėmis, sukelia randų audinį. Kepenų ląstelės, kurios nemiršta, dauginasi, bandydamos pakeisti žuvusias ląsteles. Dėl to rando audinyje susidaro naujai susiformavusių kepenų ląstelių sankaupos (regeneraciniai mazgeliai). Yra daug cirozės priežasčių, įskaitant chemines medžiagas (pvz., alkoholis, riebalus ir tam tikrus vaistus), virusus, toksiškus metalus (pvz., geležį ir varį, kurie kaupiasi kepenyse dėl genetinių ligų) ir autoimuninę kepenų ligą, kurios metu organizmo imuninė sistema atakuoja kepenis.
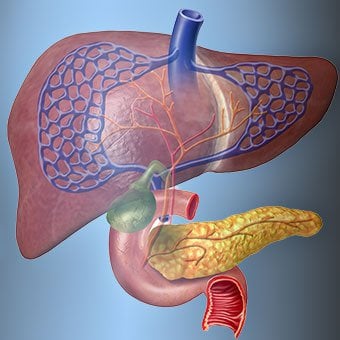
 Kepenų ir kraujo ryšys yra unikalus.
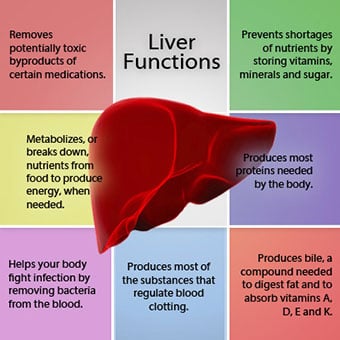
Kepenų ir kraujo ryšys yra unikalus. Kepenys yra svarbus organas organizme. Jis atlieka daug svarbių funkcijų, iš kurių dvi yra organizmui reikalingų medžiagų gamyba, pavyzdžiui, krešėjimo baltymai, būtini, kad kraujas krešėtų, ir toksinių medžiagų, kurios gali būti kenksmingos organizmui, pvz., vaistų, pašalinimas. . Kepenys taip pat atlieka svarbų vaidmenį reguliuojant gliukozės (cukraus) ir lipidų (riebalų), kuriuos organizmas naudoja kaip kurą, tiekimą. Kad galėtų atlikti šias svarbias funkcijas, kepenų ląstelės turi veikti normaliai ir būti arti kraujo, nes medžiagos, kurias prideda arba pašalina kepenys, kraujas perneša į kepenis ir iš jų. P>
Kepenų santykis su krauju yra unikalus. Skirtingai nuo daugelio kūno organų, arterijomis į kepenis tiekiamas tik nedidelis kraujo kiekis. Didžioji dalis kepenų aprūpinimo krauju gaunama iš žarnyno venų, kai kraujas grįžta į širdį. Pagrindinė vena, grąžinanti kraują iš žarnyno, vadinama vartų vena. Kai vartų vena praeina per kepenis, ji skyla į vis mažesnes ir mažesnes venas. Mažiausios venos (dėl savo unikalios struktūros vadinamos sinusoidėmis) glaudžiai liečiasi su kepenų ląstelėmis. Kepenų ląstelės išsidėsto išilgai sinusoidų. Šis glaudus ryšys tarp kepenų ląstelių ir kraujo iš vartų venos leidžia kepenų ląstelėms pašalinti ir pridėti medžiagų į kraują. Kai kraujas praeina pro sinusoidus, jis surenkamas į vis didesnes ir didesnes venas, kurios galiausiai sudaro vieną veną, kepenų veną, kuri grąžina kraują į širdį.
Sergant ciroze, sunaikinamas ryšys tarp kraujo ir kepenų ląstelių. Nors išgyvenusios arba naujai susiformavusios kepenų ląstelės gali gaminti ir pašalinti iš kraujo medžiagas, jos neturi normalaus, glaudaus ryšio su krauju, o tai trukdo kepenų ląstelių gebėjimui pridėti ar pašalinti medžiagas. nuo kraujo. Be to, randai, esantys ciroze sergančiose kepenyse, trukdo kraujui tekėti per kepenis ir į kepenų ląsteles. Dėl kliūčių kraujui tekėti per kepenis kraujas „atsitraukia“ į vartų veną ir padidėja slėgis vartų venoje, o tai vadinama portaline hipertenzija. Dėl tekėjimo kliūčių ir didelio slėgio vartų venoje kraujas vartų venoje ieško kitų venų, kuriose grįžtų į širdį, venų su mažesniu slėgiu, kurios apeina kepenis. Deja, kepenys negali pridėti ar pašalinti iš kraujo medžiagų, kurios jas apeina. Tai yra sumažėjusio kepenų ląstelių skaičiaus, normalaus per kepenis einančio kraujo ir kepenų ląstelių kontakto bei kepenis apeinančio kraujo praradimo derinys, dėl kurio atsiranda daug cirozės požymių.
Antroji cirozės sukeltų problemų priežastis – sutrikęs ryšys tarp kepenų ląstelių ir kanalų, kuriais teka tulžis. Tulžis yra kepenų ląstelių gaminamas skystis, turintis dvi svarbias funkcijas:padėti virškinti ir pašalinti bei pašalinti iš organizmo toksines medžiagas. Kepenų ląstelių gaminama tulžis išskiriama į labai mažus kanalus, kurie eina tarp kepenų ląstelių, išklojusių sinusoidus, vadinamus kanalėliais. Kanaliukai ištuštėja į mažus latakus, kurie vėliau susijungia ir sudaro vis didesnius latakus. Visi latakai susijungia į vieną lataką, kuris patenka į plonąją žarną, kur gali padėti virškinti maistą. Tuo pačiu metu tulžyje esančios toksinės medžiagos patenka į žarnyną, o vėliau pašalinamos su išmatomis. Sergant ciroze, kanalai yra nenormalūs ir sunaikinamas ryšys tarp kepenų ląstelių ir kanalėlių, kaip ir ryšys tarp kepenų ląstelių ir kraujo sinusoidėse. Dėl to kepenys nepajėgia normaliai pašalinti toksinių medžiagų, jos gali kauptis organizme. Šiek tiek susilpnėja ir virškinimas žarnyne.
 Dažni cirozės simptomai ir požymiai yra gelta, nuovargis, silpnumas, apetito praradimas, niežulys ir lengvos mėlynės.
Dažni cirozės simptomai ir požymiai yra gelta, nuovargis, silpnumas, apetito praradimas, niežulys ir lengvos mėlynės. Žmonėms, sergantiems ciroze, gali būti nedaug arba visai nėra kepenų ligos simptomų ir požymių. Kai kurie simptomai gali būti nespecifiniai ir nereiškia, kad jų priežastis yra kepenys. Dažni cirozės simptomai ir požymiai:
Žmonėms, sergantiems kepenų ciroze, taip pat atsiranda simptomų ir požymių dėl ligos komplikacijų.
Pati cirozė jau yra vėlyvoji kepenų pažeidimo stadija. Ankstyvosiose kepenų ligos stadijose bus kepenų uždegimas. Jei šis uždegimas negydomas, gali atsirasti randų (fibrozės). Šiame etape gydant kepenys vis dar gali išgyti.
Jei kepenų fibrozė negydoma, ji gali sukelti cirozę. Šiame etape rando audinys negali išgyti, tačiau randų progresavimą galima užkirsti kelią arba jį sulėtinti. Žmonėms, sergantiems ciroze, kuriems yra komplikacijų požymių, gali išsivystyti paskutinės stadijos kepenų liga (ESLD), o vienintelis gydymas šioje stadijoje yra kepenų transplantacija.
 Edema, ascitas ir bakterinio peritonito komplikacijos
Edema, ascitas ir bakterinio peritonito komplikacijos Kai kepenų cirozė tampa sunki, inkstams siunčiami signalai, kad jie sulaikytų druską ir vandenį organizme. Druskos ir vandens perteklius pirmiausia kaupiasi audinyje po kulkšnių ir kojų oda dėl gravitacijos poveikio stovint ar sėdint. Toks skysčių susikaupimas vadinamas periferine edema arba duobių edema. (Dėlinė edema reiškia faktą, kad piršto galiuku tvirtai prispaudus prie kulkšnies ar kojos su edema, odoje atsiranda įdubimas, kuris išlieka kurį laiką po spaudimo. Bet koks spaudimas, pvz., nuo elastinės kojinės juostos , gali pakakti, kad atsirastų duobių.) Patinimas dažnai pablogėja dienos pabaigoje po stovėjimo ar sėdėjimo ir gali sumažėti per naktį gulint. Kai cirozė paūmėja ir sulaikoma daugiau druskos bei vandens, pilvo ertmėje tarp pilvo sienelės ir pilvo organų gali kauptis skystis (vadinamas ascitu), sukeldamas pilvo patinimą, diskomfortą pilve ir padidėjusį svorį.
Skystis pilvo ertmėje (ascitas) yra puiki vieta bakterijoms daugintis. Paprastai pilvo ertmėje yra labai mažas skysčių kiekis, kuris gali gerai atsispirti infekcijai, o bakterijos, patekusios į pilvą (dažniausiai iš žarnyno), žūva arba patenka į vartų veną ir į kepenis, kur jos žūva. Sergant ciroze, pilve besikaupiantis skystis negali normaliai atsispirti infekcijai. Be to, daugiau bakterijų patenka iš žarnyno į ascitą. Tikėtina, kad gali atsirasti infekcija pilvo ertmėje ir ascitas, vadinamas spontaniniu bakteriniu peritonitu arba SBP. SBP yra gyvybei pavojinga komplikacija. Kai kuriems pacientams, sergantiems SBP, nėra jokių simptomų, o kitiems karščiuoja, šaltkrėtis, pilvo skausmas ir jautrumas, viduriavimas ir pablogėjęs ascitas.
 Kraujavimas ir blužnies komplikacijos
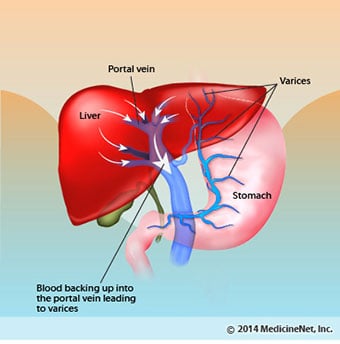
Kraujavimas ir blužnies komplikacijos Sergant ciroze, randinis audinys blokuoja iš žarnyno į širdį grįžtančio kraujo tekėjimą ir padidina spaudimą vartų venoje (portalinė hipertenzija). Kai slėgis vartų venoje tampa pakankamai didelis, kraujas tekėja aplink kepenis mažesnio slėgio venomis, kad pasiektų širdį. Dažniausios venos, kuriomis kraujas apeina kepenis, yra apatinę stemplės dalį ir viršutinę skrandžio dalį dengiančios venos.
Dėl padidėjusio kraujotakos ir dėl to padidėjusio slėgio venos apatinėje stemplės ir viršutinėje skrandžio dalyje plečiasi ir vėliau vadinamos stemplės ir skrandžio varikoze; kuo didesnis slėgis portale, tuo didesnės venų varikozės ir tuo didesnė tikimybė, kad pacientas kraujuos iš venų varikozės į stemplę arba skrandį.
Kraujavimas iš venų varikozės yra sunkus ir be neatidėliotino gydymo gali būti mirtinas. Kraujavimo iš venų varikozės simptomai yra vėmimas krauju (jis gali atrodyti kaip raudonas kraujas, susimaišęs su krešuliais arba „kavos tirščiais“), juodos ir degutinės išmatos dėl kraujo pokyčių, kai jis praeina per žarnyną (melena), ir ortostatinės išmatos. galvos svaigimas arba alpimas (sukeltas kraujospūdžio sumažėjimo, ypač atsistojus iš gulimos padėties).
Retai gali kraujuoti iš venų varikozės, susidarančių kitose žarnyno vietose, pavyzdžiui, gaubtinės žarnos. Pacientai, hospitalizuoti dėl aktyviai kraujuojančių stemplės venų varikozės, turi didelę spontaninio bakterinio peritonito atsiradimo riziką, nors to priežastys dar nėra suprantamos.
Blužnis paprastai veikia kaip filtras, pašalinantis senesnius raudonuosius kraujo kūnelius, baltuosius kraujo kūnelius ir trombocitus (mažas daleles, svarbias kraujo krešėjimui). Iš blužnies nutekėjęs kraujas prisijungia prie vartų venos iš žarnyno. Kai sergant ciroze padidėja slėgis vartų venoje, ji vis labiau blokuoja kraujo tekėjimą iš blužnies. Kraujas „atsitraukia“, kaupiasi blužnyje, o blužnis išsipučia, o tai vadinama splenomegalija. Kartais blužnis taip padidėja, kad sukelia pilvo skausmą.
Kai blužnis didėja, ji išfiltruoja vis daugiau kraujo ląstelių ir trombocitų, kol jų skaičius kraujyje sumažėja. Hipersplenizmas yra terminas, vartojamas šiai būklei apibūdinti, ir jis yra susijęs su mažu raudonųjų kraujo kūnelių skaičiumi (anemija), mažu baltųjų kraujo kūnelių skaičiumi (leukopenija) ir (arba) mažu trombocitų skaičiumi (trombocitopenija). Anemija gali sukelti silpnumą, leukopenija gali sukelti infekcijas, o trombocitopenija gali sutrikdyti kraujo krešėjimą ir užsitęsti kraujavimą
 Kepenų (kepenų) komplikacijos
Kepenų (kepenų) komplikacijos Dėl bet kokios priežasties sukelta cirozė padidina pirminio kepenų vėžio (hepatoceliulinės karcinomos) riziką. Pirminis reiškia faktą, kad navikas atsiranda kepenyse. Antrinis kepenų vėžys yra toks, kuris atsiranda kitur organizme ir plinta (metastazuoja) į kepenis.
Dažniausi pirminio kepenų vėžio simptomai ir požymiai yra pilvo skausmas ir patinimas, kepenų padidėjimas, svorio kritimas ir karščiavimas. Be to, kepenų vėžys gali gaminti ir išskirti daugybę medžiagų, įskaitant tas, kurios padidina raudonųjų kraujo kūnelių skaičių (eritrocitozę), mažina cukraus kiekį kraujyje (hipoglikemija) ir padidina kalcio kiekį kraujyje (hiperkalcemija).
Dalį maisto baltymų, kurie nepatenka į virškinimą ir pasisavinimą, sunaudoja bakterijos, kurios paprastai būna žarnyne. Naudodamos baltymus savo reikmėms, bakterijos gamina medžiagas, kurias išskiria į žarnyną, kad vėliau būtų absorbuojamos į organizmą. Kai kurios iš šių medžiagų, pavyzdžiui, amoniakas, gali turėti toksinį poveikį smegenims. Paprastai šios toksiškos medžiagos iš žarnyno per vartų veną pernešamos į kepenis, kur pašalinamos iš kraujo ir detoksikuojamos.
Sergant ciroze, kepenų ląstelės negali normaliai funkcionuoti arba dėl to, kad yra pažeistos, arba dėl to, kad prarado įprastą ryšį su krauju. Be to, dalis vartų venos kraujo apeina kepenis per kitas venas. Dėl šių anomalijų toksinių medžiagų kepenų ląstelės negali pašalinti, o kaupiasi kraujyje.
Kai toksinės medžiagos pakankamai susikaupia kraujyje, sutrinka smegenų funkcija – tokia būklė vadinama hepatine encefalopatija. Miegojimas dieną, o ne naktį (įprasto miego modelio pasikeitimas) yra ankstyvas hepatinės encefalopatijos simptomas. Kiti simptomai yra dirglumas, nesugebėjimas susikaupti ar atlikti skaičiavimus, atminties praradimas, sumišimas ar prislėgtas sąmonės lygis. Galiausiai sunki hepatinė encefalopatija sukelia komą ir mirtį.
Dėl nuodingų medžiagų ciroze sergančių pacientų smegenys tampa labai jautrios vaistams, kuriuos paprastai filtruoja ir detoksikuoja kepenys. Gali tekti sumažinti daugelio vaistų, ypač raminamųjų ir mieguistumą skatinančių vaistų, dozes, kad būtų išvengta toksinių medžiagų kaupimosi sergant ciroze. Arba gali būti naudojami vaistai, kurių nereikia detoksikuoti ar pašalinti iš organizmo kepenyse, pvz., per inkstus pašalinamus vaistus.
Pacientams, sergantiems ciroze, gali išsivystyti hepatorenalinis sindromas. Šis sindromas yra rimta komplikacija, kurios metu susilpnėja inkstų funkcija. Tai yra funkcinė inkstų problema, o tai reiškia, kad inkstai nėra fiziškai pažeisti. Vietoj to, sumažėjusi funkcija atsiranda dėl kraujo tekėjimo per pačius inkstus pokyčių. Hepatorenalinis sindromas apibrėžiamas kaip progresuojantis inkstų nepakankamumas, kurio metu organizmas nepašalina medžiagų iš kraujo ir nepagamina pakankamo šlapimo kiekio, o kitos svarbios inkstų funkcijos, pvz., druskos sulaikymas, išlieka. Jei ligoniui, sergančiam hepatorenaliniu sindromu, pagerėja kepenų funkcija arba persodinamos sveikos kepenys, inkstai dažniausiai vėl pradeda normaliai dirbti. Tai rodo, kad susilpnėjusi inkstų funkcija atsiranda dėl toksinių medžiagų kaupimosi kraujyje arba dėl nenormalios kepenų funkcijos, kai kepenys sutrinka. Yra dviejų tipų hepatorenalinis sindromas. Vienas tipas atsiranda palaipsniui per mėnesius. Kitas įvyksta greitai per savaitę ar dvi.
Retai kai kuriems pacientams, sergantiems pažengusia ciroze, gali išsivystyti hepatopulmoninis sindromas. Šiems pacientams gali pasunkėti kvėpavimas, nes kai kurie hormonai, išsiskiriantys sergant pažengusia ciroze, sukelia nenormalią plaučių funkciją. Pagrindinė plaučių problema yra ta, kad per mažas plaučių kraujagysles, kurios liečiasi su plaučių alveolėmis (oro maišeliais), teka nepakankamai kraujo. Kraujas, tekantis per plaučius, yra šuntuojamas aplink alveoles ir negali paimti pakankamai deguonies iš alveolėse esančio oro. Dėl to pacientas jaučia dusulį, ypač fizinio krūvio metu.
 Yra 12 dažniausiai pasitaikančių cirozės priežasčių.
Yra 12 dažniausiai pasitaikančių cirozės priežasčių. Dažnos priežastys of cirrhosis of the liver include:
Less common causes of cirrhosis include:
In certain parts of the world (particularly Northern Africa), infection of the liver with a parasite (schistosomiasis) is the most common cause of liver disease and cirrhosis.
 Alcohol and nonalcoholic fatty liver disease are common causes of cirrhosis.
Alcohol and nonalcoholic fatty liver disease are common causes of cirrhosis. Alcohol is a very common cause of cirrhosis, particularly in the Western world. Chronic, high levels of alcohol consumption injure liver cells. Thirty percent of individuals who drink daily at least eight to sixteen ounces of hard liquor or the equivalent for fifteen or more years will develop cirrhosis. Alcohol causes a range of liver diseases, which include simple and uncomplicated fatty liver (steatosis), more serious fatty liver with inflammation (steatohepatitis or alcoholic hepatitis), and cirrhosis.
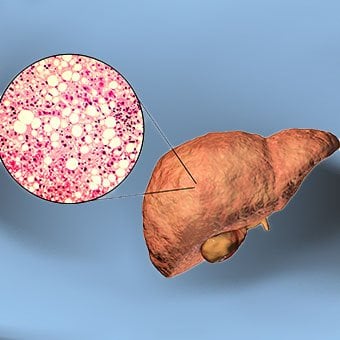
Nonalcoholic fatty liver disease (NAFLD) refers to a wide spectrum of liver diseases that, like alcoholic liver disease, range from simple steatosis, to nonalcoholic steatohepatitis (NASH), to cirrhosis. All stages of NAFLD have in common the accumulation of fat in liver cells. The term nonalcoholic is used because NAFLD occurs in individuals who do not consume excessive amounts of alcohol, yet in many respects the microscopic picture of NAFLD is similar to what can be seen in liver disease that is due to excessive alcohol. NAFLD is associated with a condition called insulin resistance, which, in turn, is associated with metabolic syndrome and diabetes mellitus type 2. Obesity is the main cause of insulin resistance, metabolic syndrome, and type 2 diabetes. NAFLD is the most common liver disease in the United States and is responsible for up to 25% of all liver disease. The number of livers transplanted for NAFLD-related cirrhosis is on the rise. Public health officials are worried that the current epidemic of obesity will dramatically increase the development of NAFLD and cirrhosis in the population.
 Primary biliary cirrhosis (PBC) is a liver disease caused by an abnormality of the immune system that is found predominantly in women.
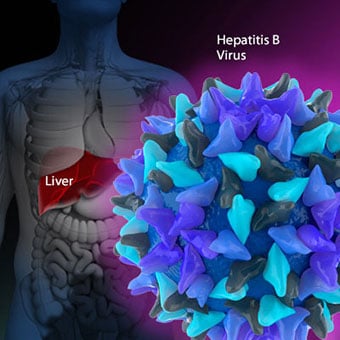
Primary biliary cirrhosis (PBC) is a liver disease caused by an abnormality of the immune system that is found predominantly in women. Chronic viral hepatitis is a condition in which hepatitis B or hepatitis C virus infects the liver for years. Most patients with viral hepatitis will not develop chronic hepatitis and cirrhosis. The majority of patients infected with hepatitis A recover completely within weeks, without developing chronic infection. In contrast, some patients infected with hepatitis B virus and most patients infected with hepatitis C virus develop chronic hepatitis, which, in turn, causes progressive liver damage and leads to cirrhosis, and, sometimes, liver cancers.
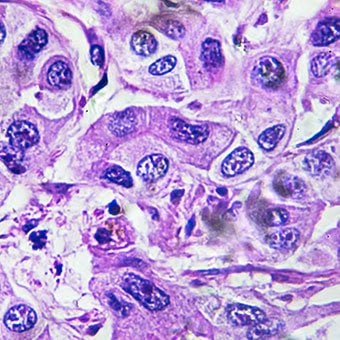
Autoimmune hepatitis is a liver disease found more commonly in women that is caused by an abnormality of the immune system. The abnormal immune activity in autoimmune hepatitis causes progressive inflammation and destruction of liver cells (hepatocytes), leading ultimately to cirrhosis.
Primary biliary cirrhosis (PBC) is a liver disease caused by an abnormality of the immune system that is found predominantly in women. The abnormal immunity in PBC causes chronic inflammation and destruction of the small bile ducts within the liver. The bile ducts are passages within the liver through which bile travels to the intestine. Bile is a fluid produced by the liver that contains substances required for digestion and absorption of fat in the intestine, as well as other compounds that are waste products, such as the pigment bilirubin. (Bilirubin is produced by the breakdown of hemoglobin from old red blood cells.). Along with the gallbladder, the bile ducts make up the biliary tract. In PBC, the destruction of the small bile ducts blocks the normal flow of bile into the intestine. As the inflammation continues to destroy more of the bile ducts, it also spreads to destroy nearby liver cells. As the destruction of the hepatocytes proceeds, scar tissue (fibrosis) forms and spreads throughout the areas of destruction. The combined effects of progressive inflammation, scarring, and the toxic effects of accumulating waste products culminates in cirrhosis.
Primary sclerosing cholangitis (PSC) is an uncommon disease frequently found in patients with Crohn's disease and ulcerative colitis. In PSC, the large bile ducts outside of the liver become inflamed, narrowed, and obstructed. Obstruction to the flow of bile leads to infections of the bile ducts and jaundice, eventually causing cirrhosis. In some patients, injury to the bile ducts (usually because of surgery) also can cause obstruction and cirrhosis of the liver.
 Different liver diseases should be diagnosed by specialists and different tests such as liver blood test, biopsy, and others.
Different liver diseases should be diagnosed by specialists and different tests such as liver blood test, biopsy, and others. Inherited (genetic) disorders that result in the accumulation of toxic substances in the liver, which leads to tissue damage and cirrhosis. Examples include the abnormal accumulation of iron (hemochromatosis) or copper (Wilson disease). In hemochromatosis, patients inherit a tendency to absorb an excessive amount of iron from food. Over time, iron accumulation in different organs throughout the body causes cirrhosis, arthritis, heart muscle damage leading to heart failure, and testicular dysfunction causing loss of sexual drive. Treatment is aimed at preventing damage to organs by removing iron from the body through phlebotomy (removing blood). In Wilson disease, there is an inherited abnormality in one of the proteins that control copper in the body. Over time, copper accumulates in the liver, eyes, and brain. Cirrhosis, tremor, psychiatric disturbances, and other neurological difficulties occur if the condition is not treated early. Treatment is with oral medication, which increases the amount of copper that is eliminated from the body in the urine.
Cryptogenic cirrhosis (cirrhosis due to unidentified causes) is a common reason for liver transplantation. It is termed called cryptogenic cirrhosis because for many years doctors have been being unable to explain why a proportion of patients developed cirrhosis. Doctors now believe that cryptogenic cirrhosis is due to NASH (nonalcoholic steatohepatitis) caused by long-standing obesity, type 2 diabetes, and insulin resistance. The fat in the liver of patients with NASH is believed to disappear with the onset of cirrhosis, and this has made it difficult for doctors to make the connection between NASH and cryptogenic cirrhosis for a long time. One important clue that NASH leads to cryptogenic cirrhosis is the finding of a high occurrence of NASH in the new livers of patients undergoing liver transplant for cryptogenic cirrhosis. Finally, a study from France suggests that patients with NASH have a similar risk of developing cirrhosis as patients with long-standing infection with hepatitis C virus. (See discussion that follows.) However, the progression to cirrhosis from NASH is thought to be slow and the diagnosis of cirrhosis typically is made in people in their sixties.
Infants can be born without bile ducts (biliary atresia) and ultimately develop cirrhosis. Other infants are born lacking vital enzymes for controlling sugars that lead to the accumulation of sugars and cirrhosis. On rare occasions, the absence of a specific enzyme can cause cirrhosis and scarring of the lung (alpha-1 antitrypsin deficiency).
Less common causes of cirrhosis include unusual reactions to some drugs and prolonged exposure to toxins, as well as chronic heart failure (cardiac cirrhosis). In certain parts of the world (particularly Northern Africa), infection of the liver with a parasite (schistosomiasis) is the most common cause of liver disease and cirrhosis.
Different liver diseases should be diagnosed by specialists and different tests such as liver blood test, biopsy, and others. The single best test for diagnosing cirrhosis is a biopsy of the liver. Liver biopsies carry a small risk for serious complications, and biopsy often is reserved for those patients in whom the diagnosis of the type of liver disease or the presence of cirrhosis is not clear. The history, physical examination, or routine testing may suggest the possibility of cirrhosis. If cirrhosis is present, other tests can be used to determine the severity of the cirrhosis and the presence of complications. Tests also may be used to diagnose the underlying disease that is causing the cirrhosis. Examples of how doctors diagnose and evaluate cirrhosis are:
 There are four types of treatment of cirrhosis.
There are four types of treatment of cirrhosis. Treatment of cirrhosis includes
Consume a balanced diet and one multivitamin daily. Patients with PBC with impaired absorption of fat-soluble vitamins may need additional vitamins D and K.
Avoid drugs (including alcohol) that cause liver damage. All patients with cirrhosis should avoid alcohol. Most patients with alcohol-induced cirrhosis experience an improvement in liver function with abstinence from alcohol. Even patients with chronic hepatitis B and C can substantially reduce liver damage and slow the progression towards cirrhosis with abstinence from alcohol.
Avoid nonsteroidal anti-inflammatory drugs (NSAIDs, e.g., ibuprofen). Patients with cirrhosis can experience worsening of liver and kidney function with NSAIDs.
Eradicate hepatitis B and hepatitis C virus by using anti-viral medications. Not all patients with cirrhosis due to chronic viral hepatitis are candidates for drug treatment. Some patients may experience serious deterioration in liver function and/or intolerable side effects during treatment. Thus, decisions to treat viral hepatitis have to be individualized, after consulting with doctors experienced in treating liver diseases (hepatologists).
Remove blood from patients with hemochromatosis to reduce the levels of iron and prevent further damage to the liver. In Wilson's disease, medications can be used to increase the excretion of copper in the urine to reduce the levels of copper in the body and prevent further damage to the liver.
Suppress the immune system with drugs such as prednisone and azathioprine (Imuran) to decrease inflammation of the liver in autoimmune hepatitis.
Treat patients with PBC with a bile acid preparation, ursodeoxycholic acid (UDCA), also called ursodiol (Actigall). Results of an analysis that combined the results from several clinical trials showed that UDCA increased survival among PBC patients during 4 years of therapy. The development of portal hypertension also was reduced by the UDCA. It is important to note that despite producing clear benefits, UDCA treatment primarily retards progression and does not cure PBC. Other medications such as colchicine and methotrexate also may have benefits in subsets of patients with PBC.
Immunize patients with cirrhosis against infection with hepatitis A and B to prevent a serious deterioration in liver. There are currently no vaccines available for immunizing against hepatitis C.
 Treatment for edema, ascites, and hypersplenism complications.
Treatment for edema, ascites, and hypersplenism complications. Retaining salt and water can lead to swelling of the ankles and legs (edema) or abdomen (ascites) in patients with cirrhosis. Doctors often advise patients with cirrhosis to restrict dietary salt (sodium) and fluid to decrease edema and ascites. The amount of salt in the diet usually is restricted to 2 grams per day and fluid to 1.2 liters per day. In most patients with cirrhosis, salt and fluid restriction is not enough and diuretics have to be added.
Diuretics are medications that work in the kidneys to promote the elimination of salt and water into the urine. A combination of the diuretics spironolactone (Aldactone) and furosemide (Lasix) can reduce or eliminate the edema and ascites in most patients. During treatment with diuretics, it is important to monitor the function of the kidneys by measuring blood levels of blood urea nitrogen (BUN) and creatinine to determine if too much diuretic is being used. Too much diuretic can lead to kidney dysfunction that is reflected in elevations of the BUN and creatinine levels in the blood.
Sometimes, when the diuretics do not work (in which case the ascites is said to be refractory), a long needle or catheter is used to draw out the ascitic fluid directly from the abdomen, a procedure called abdominal paracentesis. It is common to withdraw large amounts (liters) of fluid from the abdomen when the ascites is causing painful abdominal distension and/or difficulty breathing because it limits the movement of the diaphragms.
Another treatment for refractory ascites is a procedure called transjugular intravenous portosystemic shunting (TIPS).
The spleen normally acts as a filter to remove older red blood cells, white blood cells, and platelets (small particles important for the clotting of blood). The blood that drains from the spleen joins the blood in the portal vein from the intestines. As the pressure in the portal vein rises in cirrhosis, it increasingly blocks the flow of blood from the spleen. The blood "backs-up," accumulating in the spleen, and the spleen swells in size, a condition referred to as splenomegaly. Sometimes, the spleen is so enlarged it causes abdominal pain.
As the spleen enlarges, it filters out more and more of the blood cells and platelets until their numbers in the blood are reduced. Hypersplenism is the term used to describe this condition, and it is associated with a low red blood cell count (anemia), low white blood cell count (leukopenia), and/or a low platelet count (thrombocytopenia). Anemia can cause weakness, leucopenia can lead to infections, and thrombocytopenia can impair the clotting of blood and result in prolonged bleeding.
 Once varices have bled, they tend to rebleed and the probability that a patient will die from each bleeding episode is high (30% to 35%). Treatment is necessary to prevent the first bleeding episode as well as rebleeding.
Once varices have bled, they tend to rebleed and the probability that a patient will die from each bleeding episode is high (30% to 35%). Treatment is necessary to prevent the first bleeding episode as well as rebleeding. If large varices develop in the esophagus or upper stomach, patients with cirrhosis are at risk for serious bleeding due to rupture of these varices. Once varices have bled, they tend to rebleed and the probability that a patient will die from each bleeding episode is high (30% to 35%). Treatment is necessary to prevent the first bleeding episode as well as rebleeding. Treatments include medications and procedures to decrease the pressure in the portal vein and procedures to destroy the varices.
 Hepatic encephalopathy usually should be treated with a low protein diet and oral lactulose.
Hepatic encephalopathy usually should be treated with a low protein diet and oral lactulose. Patients with an abnormal sleep cycle, impaired thinking, odd behavior, or other signs of hepatic encephalopathy usually should be treated with a low protein diet and oral lactulose. Dietary protein is restricted because it is a source of toxic compounds that cause hepatic encephalopathy. Lactulose, which is a liquid, traps toxic compounds in the colon so they cannot be absorbed into the bloodstream, and thus cause encephalopathy. Lactulose is converted to lactic acid in the colon, and the acidic environment that results is believed to trap the toxic compounds produced by the bacteria. To be sure adequate lactulose is present in the colon at all times, the patient should adjust the dose to produce 2 to 3 semiformed bowel movements a day. Lactulose is a laxative, and the effectiveness of treatment can be judged by loosening or increasing the frequency of stools. Rifaximin (Xifaxan) is an antibiotic taken orally that is not absorbed into the body but rather remains in the intestines. It is the preferred mode of treatment of hepatic encephalopathy. Antibiotics work by suppressing the bacteria that produce the toxic compounds in the colon.
 Most patients with spontaneous bacterial peritonitis are hospitalized and treated with intravenous antibiotics.
Most patients with spontaneous bacterial peritonitis are hospitalized and treated with intravenous antibiotics. Patients suspected of having spontaneous bacterial peritonitis usually will undergo paracentesis. The fluid that is removed is examined for white blood cells and cultured for bacteria. Culturing involves inoculating a sample of the ascites into a bottle of nutrient-rich fluid that encourages the growth of bacteria, thus facilitating the identification of even small numbers of bacteria. Blood and urine samples also are often obtained for culturing because many patients with spontaneous bacterial peritonitis also will have infections in their blood and urine. Many doctors believe the infection may have begun in the blood and the urine and spread to the ascitic fluid to cause spontaneous bacterial peritonitis. Most patients with spontaneous bacterial peritonitis are hospitalized and treated with intravenous antibiotics such as cefotaxime (Claforan). Patients usually treated with antibiotics include:
Spontaneous bacterial peritonitis is a serious infection. It often occurs in patients with advanced cirrhosis whose immune systems are weak, but with modern antibiotics and early detection and treatment, the prognosis of recovering from an episode of spontaneous bacterial peritonitis is good.
In some patients, oral antibiotics (norfloxacin [Noroxin] or sulfamethoxazole and trimethoprim [Bactrim]) can be prescribed to prevent spontaneous bacterial peritonitis. Not all patients with cirrhosis and ascites should be treated with antibiotics to prevent spontaneous bacterial peritonitis, but some patients are at high risk for developing spontaneous bacterial peritonitis and warrant preventive treatment.
 The prognosis and life expectancy for cirrhosis of the liver varies and depends on the cause, the severity, any complications, and any underlying diseases.
The prognosis and life expectancy for cirrhosis of the liver varies and depends on the cause, the severity, any complications, and any underlying diseases. Several types of liver disease that cause cirrhosis (such as hepatitis B and C) are associated with a high incidence of liver cancer. It is useful to screen for liver cancer in patients with cirrhosis, as early surgical treatment or transplantation of the liver can cure the patient of cancer. The difficulty is that the methods available for screening are only partially effective, identifying at best only half of patients at a curable stage of their cancer. Despite the partial effectiveness of screening, most patients with cirrhosis, particularly hepatitis B and C, are screened yearly or every six months with ultrasound examination of the liver and measurements of cancer-produced proteins in the blood, for example, alpha-fetoprotein.
Cirrhosis is irreversible. Liver function usually gradually worsens despite treatment, and complications of cirrhosis increase and become difficult to treat. When cirrhosis is far advanced liver transplantation often is the only option for treatment. Recent advances in surgical transplantation and medications to prevent infection and rejection of the transplanted liver have greatly improved survival after transplantation. On average, more than 80% of patients who receive transplants are alive after five years. Not everyone with cirrhosis is a candidate for transplantation. Furthermore, there is a shortage of livers to transplant, and they're usually is a long (months to years) wait before a liver for transplanting becomes available. Measures to slow the progression of liver disease, and treat and prevent complications of cirrhosis are vitally important.
The prognosis and life expectancy for cirrhosis of the liver varies and depends on the cause, the severity, any complications, and any underlying diseases.
Progress in the management and prevention of cirrhosis continues. Research is ongoing to determine the mechanism of scar formation in the liver and how this process of scarring can be interrupted or even reversed. Newer and better treatments for viral liver disease are being developed to prevent the progression to cirrhosis. Prevention of viral hepatitis by vaccination, which is available for hepatitis B, is being developed for hepatitis C. Treatments for the complications of cirrhosis are being developed or revised, and tested continually. Finally, research is being directed at identifying new proteins in the blood that can detect liver cancer early or predict which patients will develop liver cancer.
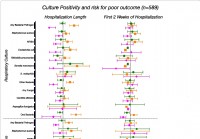 Mikrobai galėjo numatyti mirtinus rezultatus vėdinamiems COVID-19 pacientams
Buvimas Mikoplazmos seilių ventiliuojamų pacientų, sergančių COVID-19 infekcija, apatiniuose kvėpavimo takuose yra susijęs su padidėjusia mirties tikimybe. Rezultatas buvo molekulinio tyrimo dalis,
Mikrobai galėjo numatyti mirtinus rezultatus vėdinamiems COVID-19 pacientams
Buvimas Mikoplazmos seilių ventiliuojamų pacientų, sergančių COVID-19 infekcija, apatiniuose kvėpavimo takuose yra susijęs su padidėjusia mirties tikimybe. Rezultatas buvo molekulinio tyrimo dalis,
 Daugiau žmonių reikia išmokyti vartoti epinefriną gelbstintiems žmonėms, teigia advokatai
Naujausios alergijos naujienos Lietus ar šviečia, alergijos yra sunkios. Pasirūpinkite, kad astma, alergija kontroliuotų jūsų sprendimą Šiais metais atostogos bus be alergijos Mamos svoris prieš nėšt
Daugiau žmonių reikia išmokyti vartoti epinefriną gelbstintiems žmonėms, teigia advokatai
Naujausios alergijos naujienos Lietus ar šviečia, alergijos yra sunkios. Pasirūpinkite, kad astma, alergija kontroliuotų jūsų sprendimą Šiais metais atostogos bus be alergijos Mamos svoris prieš nėšt
 Kokiu būdu geriausia pašalinti inkstų akmenis?
Retrogradinė intrarenalinė chirurgija (RIRS) yra geriausia inkstų akmenų šalinimo procedūra, kurią sudaro šie veiksmai. Inkstų akmenų gydymas priklausys nuo įvairių veiksnių, tokių kaip: Dydis Vieta
Kokiu būdu geriausia pašalinti inkstų akmenis?
Retrogradinė intrarenalinė chirurgija (RIRS) yra geriausia inkstų akmenų šalinimo procedūra, kurią sudaro šie veiksmai. Inkstų akmenų gydymas priklausys nuo įvairių veiksnių, tokių kaip: Dydis Vieta





