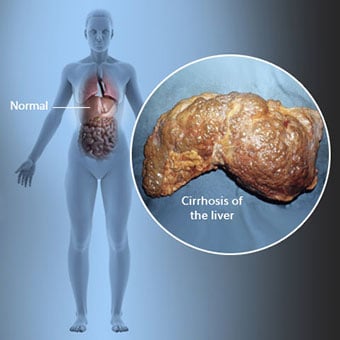
 Cirrose is een complicatie van een leverziekte die gepaard gaat met verlies van levercellen en onomkeerbare littekens in de lever.
Cirrose is een complicatie van een leverziekte die gepaard gaat met verlies van levercellen en onomkeerbare littekens in de lever. Personen met cirrose kunnen weinig of geen symptomen en tekenen van leverziekte hebben. Sommige symptomen kunnen niet-specifiek zijn, dat wil zeggen, ze suggereren niet dat de lever de oorzaak is. Enkele van de meest voorkomende symptomen en tekenen van cirrose zijn:
Personen met cirrose ontwikkelen ook symptomen en tekenen van de complicaties van cirrose.
 Er zijn veel oorzaken van cirrose, waaronder chemicaliën (zoals alcohol, vet en bepaalde medicijnen), virussen, giftige metalen en auto-immuunziekte van de lever waarbij het immuunsysteem van het lichaam de lever aanvalt.
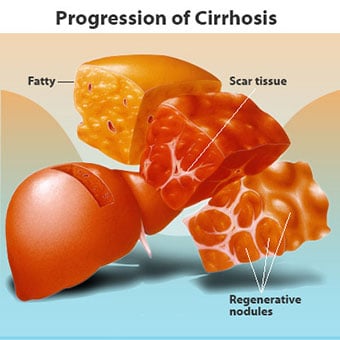
Er zijn veel oorzaken van cirrose, waaronder chemicaliën (zoals alcohol, vet en bepaalde medicijnen), virussen, giftige metalen en auto-immuunziekte van de lever waarbij het immuunsysteem van het lichaam de lever aanvalt. Cirrose is een complicatie van veel leverziekten die worden gekenmerkt door een abnormale structuur en functie van de lever. De ziekten die tot cirrose leiden, doen dat omdat ze levercellen beschadigen en doden, waarna de ontsteking en het herstel die gepaard gaan met de stervende levercellen littekenweefsel veroorzaken. De levercellen die niet afsterven vermenigvuldigen zich in een poging de afgestorven cellen te vervangen. Dit resulteert in clusters van nieuw gevormde levercellen (regeneratieve knobbeltjes) in het littekenweefsel. Er zijn veel oorzaken van cirrose, waaronder chemicaliën (zoals alcohol, vet en bepaalde medicijnen), virussen, giftige metalen (zoals ijzer en koper die zich ophopen in de lever als gevolg van genetische ziekten) en auto-immuunziekte waarbij de lever het immuunsysteem van het lichaam valt de lever aan.
 De relatie tussen de lever en het bloed is uniek.
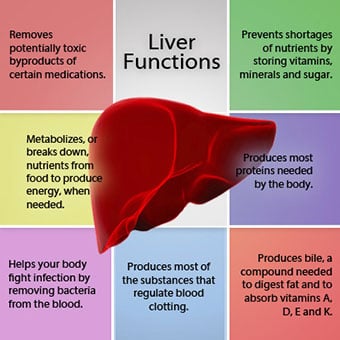
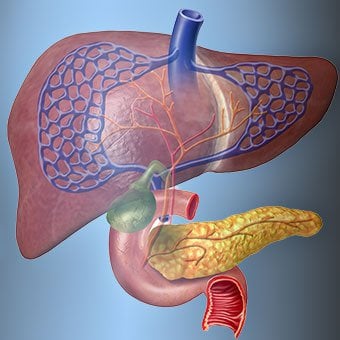
De relatie tussen de lever en het bloed is uniek. De lever is een belangrijk orgaan in het lichaam. Het vervult veel kritieke functies, waarvan er twee stoffen produceren die het lichaam nodig heeft, bijvoorbeeld het stollen van eiwitten die nodig zijn om bloed te laten stollen, en het verwijderen van giftige stoffen die schadelijk kunnen zijn voor het lichaam, zoals medicijnen . De lever speelt ook een belangrijke rol bij het reguleren van de toevoer van glucose (suiker) en lipiden (vet) die het lichaam als brandstof gebruikt. Om deze kritieke functies uit te voeren, moeten de levercellen normaal werken en moeten ze zich dicht bij het bloed bevinden, omdat de stoffen die door de lever worden toegevoegd of verwijderd door het bloed van en naar de lever worden getransporteerd.
De relatie van de lever met het bloed is uniek. In tegenstelling tot de meeste organen in het lichaam, wordt slechts een kleine hoeveelheid bloed door slagaders aan de lever geleverd. Het grootste deel van de bloedtoevoer van de lever komt uit de darmaders als het bloed terugkeert naar het hart. De hoofdader die het bloed uit de darmen terugvoert, wordt de poortader genoemd. Terwijl de poortader door de lever gaat, valt deze uiteen in steeds kleinere en kleinere aderen. De kleinste aderen (sinusoïden genoemd vanwege hun unieke structuur) staan in nauw contact met de levercellen. Levercellen liggen langs de lengte van de sinusoïden. Door deze nauwe relatie tussen de levercellen en het bloed uit de poortader kunnen de levercellen stoffen verwijderen en aan het bloed toevoegen. Als het bloed eenmaal door de sinusoïden is gestroomd, wordt het verzameld in steeds grotere en grotere aderen die uiteindelijk één enkele ader vormen, de leverader, die het bloed terugvoert naar het hart.
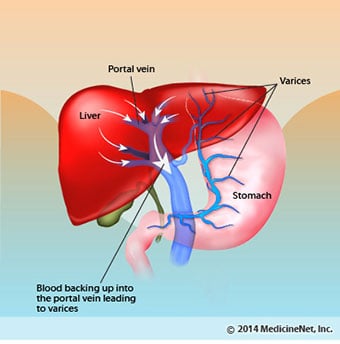
Bij cirrose wordt de relatie tussen bloed en levercellen vernietigd. Ook al kunnen de levercellen die overleven of nieuw gevormd zijn stoffen produceren en uit het bloed verwijderen, ze hebben niet de normale, intieme relatie met het bloed, en dit verstoort het vermogen van de levercellen om stoffen toe te voegen of te verwijderen. uit het bloed. Bovendien belemmert de littekenvorming in de cirrotische lever de bloedstroom door de lever en naar de levercellen. Als gevolg van de obstructie van de bloedstroom door de lever, "stapelt" het bloed zich terug in de poortader en neemt de druk in de poortader toe, een aandoening die portale hypertensie wordt genoemd. Vanwege de obstructie van de stroming en de hoge druk in de poortader, zoekt bloed in de poortader andere aderen om terug te keren naar het hart, aderen met een lagere druk die de lever omzeilen. Helaas is de lever niet in staat om stoffen toe te voegen aan of te verwijderen uit het bloed dat het omzeilt. Het is een combinatie van een verminderd aantal levercellen, verlies van het normale contact tussen bloed dat door de lever gaat en de levercellen, en bloed dat de lever omzeilt, wat leidt tot veel van de tekenen van cirrose.
Een tweede reden voor de problemen veroorzaakt door cirrose is de verstoorde relatie tussen de levercellen en de kanalen waardoor gal stroomt. Gal is een vloeistof die wordt geproduceerd door levercellen en die twee belangrijke functies heeft:helpen bij de spijsvertering en het verwijderen en elimineren van giftige stoffen uit het lichaam. De gal die door levercellen wordt geproduceerd, wordt uitgescheiden in zeer kleine kanaaltjes die tussen de levercellen lopen die de sinusoïden bekleden, genaamd canaliculi. De canaliculi monden uit in kleine kanalen die vervolgens samenkomen om steeds grotere kanalen te vormen. Alle kanalen worden samengevoegd tot één kanaal dat de dunne darm binnenkomt, waar het kan helpen bij de vertering van voedsel. Tegelijkertijd komen giftige stoffen in de gal de darm binnen en worden vervolgens geëlimineerd in de ontlasting. Bij cirrose zijn de canaliculi abnormaal en wordt de relatie tussen levercellen en canaliculi vernietigd, net als de relatie tussen de levercellen en het bloed in de sinusoïden. Als gevolg hiervan kan de lever toxische stoffen niet normaal verwijderen en kunnen ze zich ophopen in het lichaam. In mindere mate wordt ook de spijsvertering in de darm verminderd.
 Veelvoorkomende symptomen en tekenen van cirrose zijn geelzucht, vermoeidheid, zwakte, verlies van eetlust, jeuk en gemakkelijk blauwe plekken krijgen.
Veelvoorkomende symptomen en tekenen van cirrose zijn geelzucht, vermoeidheid, zwakte, verlies van eetlust, jeuk en gemakkelijk blauwe plekken krijgen. Mensen met cirrose hebben mogelijk weinig of geen symptomen en tekenen van een leverziekte. Sommige symptomen kunnen niet-specifiek zijn en suggereren niet dat de lever de oorzaak is. Veel voorkomende symptomen en tekenen van cirrose zijn:
Mensen met levercirrose ontwikkelen ook symptomen en tekenen van de complicaties van de ziekte.
Cirrose op zich is al een laat stadium van leverschade. In de vroege stadia van een leverziekte zal er een ontsteking van de lever zijn. Als deze ontsteking niet wordt behandeld, kan dit leiden tot littekens (fibrose). In dit stadium is het nog steeds mogelijk voor de lever om te genezen met de behandeling.
Als fibrose van de lever niet wordt behandeld, kan dit leiden tot cirrose. In dit stadium kan het littekenweefsel niet genezen, maar de progressie van de littekens kan worden voorkomen of vertraagd. Mensen met cirrose die tekenen van complicaties hebben, kunnen eindstadium leverziekte (ESLD) ontwikkelen en de enige behandeling in dit stadium is levertransplantatie.
 Complicaties van oedeem, ascites en bacteriële peritonitis
Complicaties van oedeem, ascites en bacteriële peritonitis Als cirrose van de lever ernstig wordt, worden signalen naar de nieren gestuurd om zout en water in het lichaam vast te houden. Het overtollige zout en water hoopt zich eerst op in het weefsel onder de huid van enkels en benen door de zwaartekracht bij het staan of zitten. Deze ophoping van vocht wordt perifeer oedeem of putjesoedeem genoemd. (Pitting oedeem verwijst naar het feit dat het stevig drukken van een vingertop tegen een enkel of been met oedeem een deuk in de huid veroorzaakt die enige tijd aanhoudt na het wegnemen van de druk. Elke vorm van druk, zoals van de elastische band van een sok , kan voldoende zijn om putjes te veroorzaken.) De zwelling is vaak erger aan het einde van de dag na staan of zitten en kan 's nachts verminderen als u ligt. Naarmate cirrose verergert en er meer zout en water worden vastgehouden, kan er zich ook vocht ophopen in de buikholte tussen de buikwand en de buikorganen (ascites genoemd), wat zwelling van de buik, buikpijn en gewichtstoename veroorzaakt.
Vloeistof in de buikholte (ascites) is de perfecte plek voor bacteriën om te groeien. Normaal gesproken bevat de buikholte een zeer kleine hoeveelheid vloeistof die infectie goed kan weerstaan, en bacteriën die de buik binnenkomen (meestal vanuit de darm) worden gedood of vinden hun weg naar de poortader en naar de lever waar ze worden gedood. Bij cirrose is de vloeistof die zich in de buik verzamelt, niet in staat om de infectie normaal te weerstaan. Daarnaast vinden meer bacteriën hun weg vanuit de darm naar de ascites. Infectie in de buik en de ascites, spontane bacteriële peritonitis of SBP genoemd, zal waarschijnlijk optreden. SBP is een levensbedreigende complicatie. Sommige patiënten met SBP hebben geen symptomen, terwijl anderen koorts, koude rillingen, buikpijn en gevoeligheid, diarree en verergering van ascites hebben.
 Bloedingen en miltcomplicaties
Bloedingen en miltcomplicaties In de cirrotische lever blokkeert het littekenweefsel de bloedstroom die vanuit de darmen naar het hart terugkeert en verhoogt het de druk in de poortader (portale hypertensie). Wanneer de druk in de poortader hoog genoeg wordt, zorgt dit ervoor dat het bloed door de lever stroomt door aderen met een lagere druk om het hart te bereiken. De meest voorkomende aderen waardoor het bloed de lever omzeilt, zijn de aderen die het onderste deel van de slokdarm en het bovenste deel van de maag bekleden.
Als gevolg van de verhoogde bloedstroom en de resulterende toename van de druk, zetten de aderen in de onderste slokdarm en de bovenste maag uit en worden dan slokdarm- en maagvarices genoemd; hoe hoger de poortdruk, hoe groter de varices en hoe groter de kans dat een patiënt uit de varices bloedt in de slokdarm of maag.
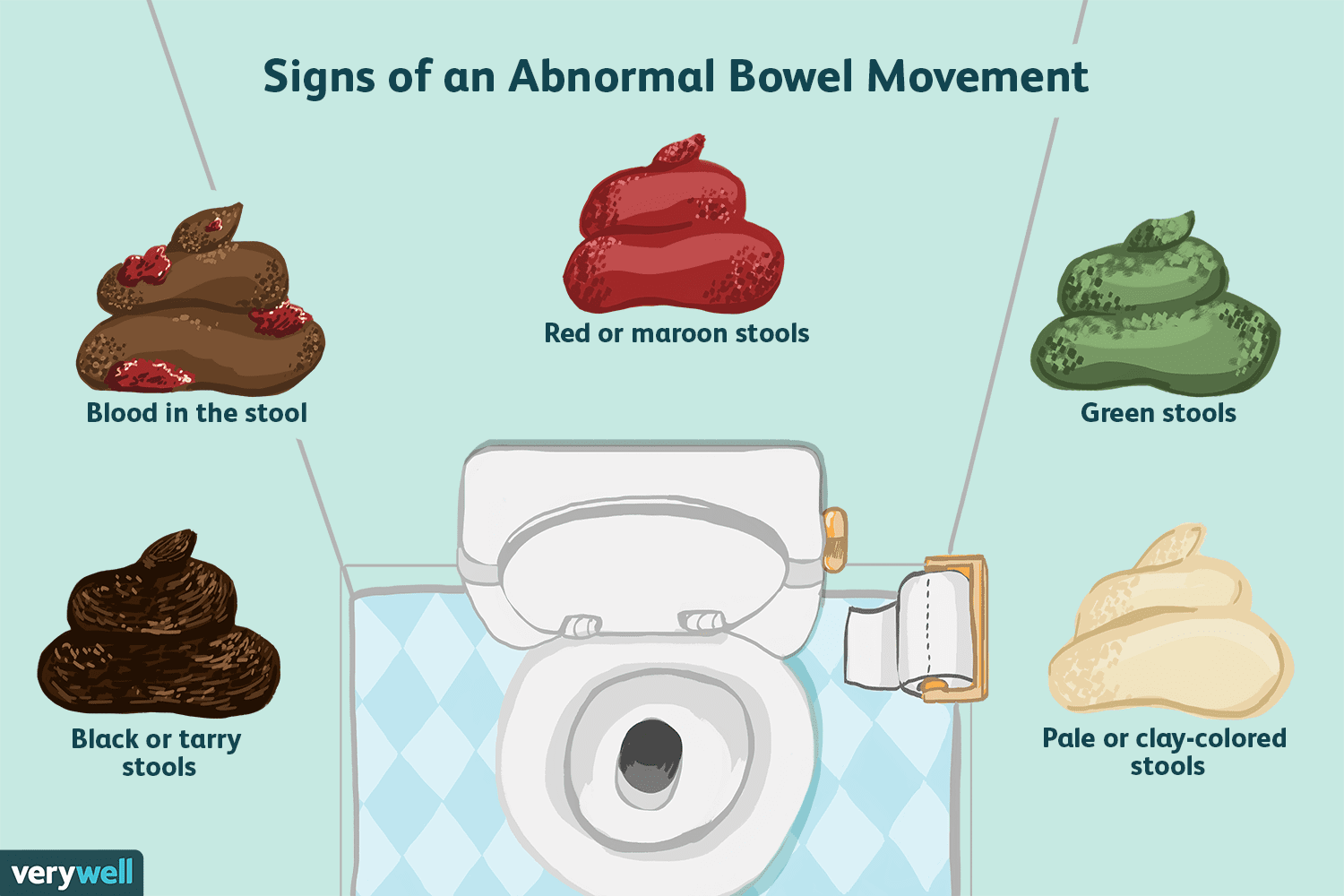
Bloeden door varices is ernstig en kan zonder onmiddellijke behandeling dodelijk zijn. Symptomen van bloedingen uit spataderen zijn onder meer bloed overgeven (het kan verschijnen als rood bloed vermengd met stolsels of "koffiedik"), ontlasting die zwart en teerachtig is als gevolg van veranderingen in het bloed terwijl het door de darm gaat (melena), en orthostatische duizeligheid of flauwvallen (veroorzaakt door een daling van de bloeddruk, vooral bij het opstaan vanuit een liggende positie).
Bloedingen kunnen zelden optreden door varices die zich elders in de darmen vormen, bijvoorbeeld de dikke darm. Patiënten die in het ziekenhuis worden opgenomen vanwege actief bloedende slokdarmvarices hebben een hoog risico op het ontwikkelen van spontane bacteriële peritonitis, hoewel de redenen hiervoor nog niet zijn begrepen.
De milt werkt normaal gesproken als een filter om oudere rode bloedcellen, witte bloedcellen en bloedplaatjes (kleine deeltjes die belangrijk zijn voor de bloedstolling) te verwijderen. Het bloed dat uit de milt stroomt, voegt zich bij het bloed in de poortader vanuit de darmen. Naarmate de druk in de poortader bij cirrose stijgt, wordt de bloedstroom uit de milt steeds meer geblokkeerd. Het bloed "back-up", zich ophopend in de milt, en de milt zwelt in omvang, een aandoening die splenomegalie wordt genoemd. Soms is de milt zo vergroot dat het buikpijn veroorzaakt.
Naarmate de milt groter wordt, filtert het steeds meer bloedcellen en bloedplaatjes totdat hun aantal in het bloed is verminderd. Hypersplenisme is de term die wordt gebruikt om deze aandoening te beschrijven en wordt geassocieerd met een laag aantal rode bloedcellen (anemie), een laag aantal witte bloedcellen (leukopenie) en/of een laag aantal bloedplaatjes (trombocytopenie). Bloedarmoede kan zwakte veroorzaken, leukopenie kan leiden tot infecties en trombocytopenie kan de bloedstolling belemmeren en leiden tot langdurige bloedingen
 Levercomplicaties (lever)
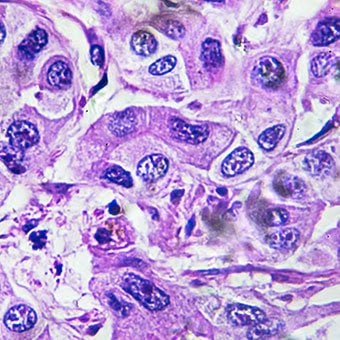
Levercomplicaties (lever) Cirrose door welke oorzaak dan ook verhoogt het risico op primaire leverkanker (hepatocellulair carcinoom). Primair verwijst naar het feit dat de tumor in de lever ontstaat. Een secundaire leverkanker is er een die ergens anders in het lichaam ontstaat en zich uitzaait (metastaseert) naar de lever.
De meest voorkomende symptomen en tekenen van primaire leverkanker zijn buikpijn en zwelling, een vergrote lever, gewichtsverlies en koorts. Bovendien kan leverkanker een aantal stoffen produceren en afgeven, waaronder stoffen die een verhoogd aantal rode bloedcellen (erythrocytose), een lage bloedsuikerspiegel (hypoglykemie) en een hoog calciumgehalte in het bloed (hypercalciëmie) veroorzaken.
Een deel van het eiwit in voedsel dat aan de spijsvertering en absorptie ontsnapt, wordt gebruikt door bacteriën die normaal in de darm aanwezig zijn. Terwijl ze het eiwit voor hun eigen doeleinden gebruiken, maken de bacteriën stoffen die ze in de darm afgeven om vervolgens in het lichaam te worden opgenomen. Sommige van deze stoffen, zoals ammoniak, kunnen toxische effecten hebben op de hersenen. Gewoonlijk worden deze giftige stoffen vanuit de darm in de poortader naar de lever vervoerd, waar ze uit het bloed worden verwijderd en ontgift.
Wanneer cirrose aanwezig is, kunnen levercellen niet normaal functioneren omdat ze beschadigd zijn of omdat ze hun normale relatie met het bloed hebben verloren. Bovendien passeert een deel van het bloed in de poortader de lever via andere aderen. Het gevolg van deze afwijkingen is dat giftige stoffen niet door de levercellen kunnen worden verwijderd, maar zich ophopen in het bloed.
Wanneer de giftige stoffen zich voldoende in het bloed ophopen, wordt de functie van de hersenen aangetast, een aandoening die hepatische encefalopathie wordt genoemd. Overdag slapen in plaats van 's nachts (omkering van het normale slaappatroon) is een vroeg symptoom van hepatische encefalopathie. Andere symptomen zijn prikkelbaarheid, onvermogen om zich te concentreren of berekeningen uit te voeren, geheugenverlies, verwardheid of verlaagde bewustzijnsniveaus. Uiteindelijk veroorzaakt ernstige hepatische encefalopathie coma en overlijden.
De giftige stoffen maken de hersenen van patiënten met cirrose ook erg gevoelig voor medicijnen die normaal gesproken door de lever worden gefilterd en ontgift. Doses van veel medicijnen moeten mogelijk worden verlaagd om een toxische opbouw bij cirrose te voorkomen, met name sedativa en medicijnen die worden gebruikt om de slaap te bevorderen. Als alternatief kunnen medicijnen worden gebruikt die niet door de lever hoeven te worden ontgift of uit het lichaam moeten worden geëlimineerd, zoals medicijnen die door de nieren worden uitgescheiden.
Patiënten met verergerende cirrose kunnen hepatorenaal syndroom ontwikkelen. Dit syndroom is een ernstige complicatie waarbij de functie van de nieren is verminderd. Het is een functioneel probleem in de nieren, wat betekent dat er geen fysieke schade aan de nieren is. In plaats daarvan is de verminderde functie te wijten aan veranderingen in de manier waarop het bloed door de nieren zelf stroomt. Het hepatorenaal syndroom wordt gedefinieerd als progressief falen van de nieren om stoffen uit het bloed te verwijderen en voldoende hoeveelheden urine te produceren, terwijl andere belangrijke functies van de nier, zoals het vasthouden van zout, behouden blijven. Als de leverfunctie verbetert of een gezonde lever wordt getransplanteerd bij een patiënt met hepatorenaal syndroom, beginnen de nieren meestal weer normaal te werken. Dit suggereert dat de verminderde functie van de nieren het gevolg is van ofwel de ophoping van giftige stoffen in het bloed of een abnormale leverfunctie wanneer de lever faalt. Er zijn twee soorten hepatorenaal syndroom. Eén type treedt geleidelijk op gedurende maanden. De andere treedt snel op gedurende een week of twee.
In zeldzame gevallen kunnen sommige patiënten met gevorderde cirrose hepatopulmonaal syndroom ontwikkelen. Deze patiënten kunnen moeite hebben met ademhalen omdat bepaalde hormonen die vrijkomen bij gevorderde cirrose ervoor zorgen dat de longen abnormaal functioneren. Het fundamentele probleem in de long is dat er niet genoeg bloed door de kleine bloedvaten in de longen stroomt die in contact staan met de longblaasjes (luchtzakjes) van de longen. Bloed dat door de longen stroomt, wordt om de longblaasjes heen geslagen en kan niet genoeg zuurstof uit de lucht in de longblaasjes opnemen. Als gevolg hiervan ervaart de patiënt kortademigheid, vooral bij inspanning.
 Er zijn 12 veelvoorkomende oorzaken van cirrose.
Er zijn 12 veelvoorkomende oorzaken van cirrose. Common causes of cirrhosis of the liver include:
Less common causes of cirrhosis include:
In certain parts of the world (particularly Northern Africa), infection of the liver with a parasite (schistosomiasis) is the most common cause of liver disease and cirrhosis.
 Alcohol and nonalcoholic fatty liver disease are common causes of cirrhosis.
Alcohol and nonalcoholic fatty liver disease are common causes of cirrhosis. Alcohol is a very common cause of cirrhosis, particularly in the Western world. Chronic, high levels of alcohol consumption injure liver cells. Thirty percent of individuals who drink daily at least eight to sixteen ounces of hard liquor or the equivalent for fifteen or more years will develop cirrhosis. Alcohol causes a range of liver diseases, which include simple and uncomplicated fatty liver (steatosis), more serious fatty liver with inflammation (steatohepatitis or alcoholic hepatitis), and cirrhosis.
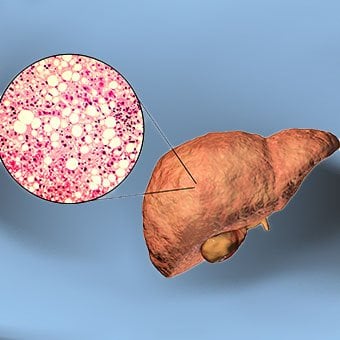
Nonalcoholic fatty liver disease (NAFLD) refers to a wide spectrum of liver diseases that, like alcoholic liver disease, range from simple steatosis, to nonalcoholic steatohepatitis (NASH), to cirrhosis. All stages of NAFLD have in common the accumulation of fat in liver cells. The term nonalcoholic is used because NAFLD occurs in individuals who do not consume excessive amounts of alcohol, yet in many respects the microscopic picture of NAFLD is similar to what can be seen in liver disease that is due to excessive alcohol. NAFLD is associated with a condition called insulin resistance, which, in turn, is associated with metabolic syndrome and diabetes mellitus type 2. Obesity is the main cause of insulin resistance, metabolic syndrome, and type 2 diabetes. NAFLD is the most common liver disease in the United States and is responsible for up to 25% of all liver disease. The number of livers transplanted for NAFLD-related cirrhosis is on the rise. Public health officials are worried that the current epidemic of obesity will dramatically increase the development of NAFLD and cirrhosis in the population.
 Primary biliary cirrhosis (PBC) is a liver disease caused by an abnormality of the immune system that is found predominantly in women.
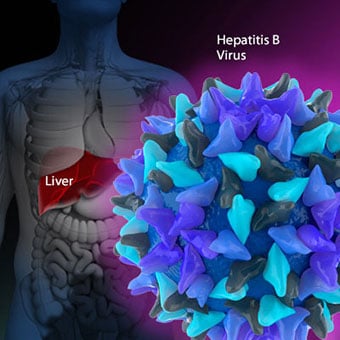
Primary biliary cirrhosis (PBC) is a liver disease caused by an abnormality of the immune system that is found predominantly in women. Chronic viral hepatitis is a condition in which hepatitis B or hepatitis C virus infects the liver for years. Most patients with viral hepatitis will not develop chronic hepatitis and cirrhosis. The majority of patients infected with hepatitis A recover completely within weeks, without developing chronic infection. In contrast, some patients infected with hepatitis B virus and most patients infected with hepatitis C virus develop chronic hepatitis, which, in turn, causes progressive liver damage and leads to cirrhosis, and, sometimes, liver cancers.
Autoimmune hepatitis is a liver disease found more commonly in women that is caused by an abnormality of the immune system. The abnormal immune activity in autoimmune hepatitis causes progressive inflammation and destruction of liver cells (hepatocytes), leading ultimately to cirrhosis.
Primary biliary cirrhosis (PBC) is a liver disease caused by an abnormality of the immune system that is found predominantly in women. The abnormal immunity in PBC causes chronic inflammation and destruction of the small bile ducts within the liver. The bile ducts are passages within the liver through which bile travels to the intestine. Bile is a fluid produced by the liver that contains substances required for digestion and absorption of fat in the intestine, as well as other compounds that are waste products, such as the pigment bilirubin. (Bilirubin is produced by the breakdown of hemoglobin from old red blood cells.). Along with the gallbladder, the bile ducts make up the biliary tract. In PBC, the destruction of the small bile ducts blocks the normal flow of bile into the intestine. As the inflammation continues to destroy more of the bile ducts, it also spreads to destroy nearby liver cells. As the destruction of the hepatocytes proceeds, scar tissue (fibrosis) forms and spreads throughout the areas of destruction. The combined effects of progressive inflammation, scarring, and the toxic effects of accumulating waste products culminates in cirrhosis.
Primary sclerosing cholangitis (PSC) is an uncommon disease frequently found in patients with Crohn's disease and ulcerative colitis. In PSC, the large bile ducts outside of the liver become inflamed, narrowed, and obstructed. Obstruction to the flow of bile leads to infections of the bile ducts and jaundice, eventually causing cirrhosis. In some patients, injury to the bile ducts (usually because of surgery) also can cause obstruction and cirrhosis of the liver.
 Different liver diseases should be diagnosed by specialists and different tests such as liver blood test, biopsy, and others.
Different liver diseases should be diagnosed by specialists and different tests such as liver blood test, biopsy, and others. Inherited (genetic) disorders that result in the accumulation of toxic substances in the liver, which leads to tissue damage and cirrhosis. Examples include the abnormal accumulation of iron (hemochromatosis) or copper (Wilson disease). In hemochromatosis, patients inherit a tendency to absorb an excessive amount of iron from food. Over time, iron accumulation in different organs throughout the body causes cirrhosis, arthritis, heart muscle damage leading to heart failure, and testicular dysfunction causing loss of sexual drive. Treatment is aimed at preventing damage to organs by removing iron from the body through phlebotomy (removing blood). In Wilson disease, there is an inherited abnormality in one of the proteins that control copper in the body. Over time, copper accumulates in the liver, eyes, and brain. Cirrhosis, tremor, psychiatric disturbances, and other neurological difficulties occur if the condition is not treated early. Treatment is with oral medication, which increases the amount of copper that is eliminated from the body in the urine.
Cryptogenic cirrhosis (cirrhosis due to unidentified causes) is a common reason for liver transplantation. It is termed called cryptogenic cirrhosis because for many years doctors have been being unable to explain why a proportion of patients developed cirrhosis. Doctors now believe that cryptogenic cirrhosis is due to NASH (nonalcoholic steatohepatitis) caused by long-standing obesity, type 2 diabetes, and insulin resistance. The fat in the liver of patients with NASH is believed to disappear with the onset of cirrhosis, and this has made it difficult for doctors to make the connection between NASH and cryptogenic cirrhosis for a long time. One important clue that NASH leads to cryptogenic cirrhosis is the finding of a high occurrence of NASH in the new livers of patients undergoing liver transplant for cryptogenic cirrhosis. Finally, a study from France suggests that patients with NASH have a similar risk of developing cirrhosis as patients with long-standing infection with hepatitis C virus. (See discussion that follows.) However, the progression to cirrhosis from NASH is thought to be slow and the diagnosis of cirrhosis typically is made in people in their sixties.
Infants can be born without bile ducts (biliary atresia) and ultimately develop cirrhosis. Other infants are born lacking vital enzymes for controlling sugars that lead to the accumulation of sugars and cirrhosis. On rare occasions, the absence of a specific enzyme can cause cirrhosis and scarring of the lung (alpha-1 antitrypsin deficiency).
Less common causes of cirrhosis include unusual reactions to some drugs and prolonged exposure to toxins, as well as chronic heart failure (cardiac cirrhosis). In certain parts of the world (particularly Northern Africa), infection of the liver with a parasite (schistosomiasis) is the most common cause of liver disease and cirrhosis.
Different liver diseases should be diagnosed by specialists and different tests such as liver blood test, biopsy, and others. The single best test for diagnosing cirrhosis is a biopsy of the liver. Liver biopsies carry a small risk for serious complications, and biopsy often is reserved for those patients in whom the diagnosis of the type of liver disease or the presence of cirrhosis is not clear. The history, physical examination, or routine testing may suggest the possibility of cirrhosis. If cirrhosis is present, other tests can be used to determine the severity of the cirrhosis and the presence of complications. Tests also may be used to diagnose the underlying disease that is causing the cirrhosis. Examples of how doctors diagnose and evaluate cirrhosis are:
 There are four types of treatment of cirrhosis.
There are four types of treatment of cirrhosis. Treatment of cirrhosis includes
Consume a balanced diet and one multivitamin daily. Patients with PBC with impaired absorption of fat-soluble vitamins may need additional vitamins D and K.
Avoid drugs (including alcohol) that cause liver damage. All patients with cirrhosis should avoid alcohol. Most patients with alcohol-induced cirrhosis experience an improvement in liver function with abstinence from alcohol. Even patients with chronic hepatitis B and C can substantially reduce liver damage and slow the progression towards cirrhosis with abstinence from alcohol.
Avoid nonsteroidal anti-inflammatory drugs (NSAIDs, e.g., ibuprofen). Patients with cirrhosis can experience worsening of liver and kidney function with NSAIDs.
Eradicate hepatitis B and hepatitis C virus by using anti-viral medications. Not all patients with cirrhosis due to chronic viral hepatitis are candidates for drug treatment. Some patients may experience serious deterioration in liver function and/or intolerable side effects during treatment. Thus, decisions to treat viral hepatitis have to be individualized, after consulting with doctors experienced in treating liver diseases (hepatologists).
Remove blood from patients with hemochromatosis to reduce the levels of iron and prevent further damage to the liver. In Wilson's disease, medications can be used to increase the excretion of copper in the urine to reduce the levels of copper in the body and prevent further damage to the liver.
Suppress the immune system with drugs such as prednisone and azathioprine (Imuran) to decrease inflammation of the liver in autoimmune hepatitis.
Treat patients with PBC with a bile acid preparation, ursodeoxycholic acid (UDCA), also called ursodiol (Actigall). Results of an analysis that combined the results from several clinical trials showed that UDCA increased survival among PBC patients during 4 years of therapy. The development of portal hypertension also was reduced by the UDCA. It is important to note that despite producing clear benefits, UDCA treatment primarily retards progression and does not cure PBC. Other medications such as colchicine and methotrexate also may have benefits in subsets of patients with PBC.
Immunize patients with cirrhosis against infection with hepatitis A and B to prevent a serious deterioration in liver. There are currently no vaccines available for immunizing against hepatitis C.
 Treatment for edema, ascites, and hypersplenism complications.
Treatment for edema, ascites, and hypersplenism complications. Retaining salt and water can lead to swelling of the ankles and legs (edema) or abdomen (ascites) in patients with cirrhosis. Doctors often advise patients with cirrhosis to restrict dietary salt (sodium) and fluid to decrease edema and ascites. The amount of salt in the diet usually is restricted to 2 grams per day and fluid to 1.2 liters per day. In most patients with cirrhosis, salt and fluid restriction is not enough and diuretics have to be added.
Diuretics are medications that work in the kidneys to promote the elimination of salt and water into the urine. A combination of the diuretics spironolactone (Aldactone) and furosemide (Lasix) can reduce or eliminate the edema and ascites in most patients. During treatment with diuretics, it is important to monitor the function of the kidneys by measuring blood levels of blood urea nitrogen (BUN) and creatinine to determine if too much diuretic is being used. Too much diuretic can lead to kidney dysfunction that is reflected in elevations of the BUN and creatinine levels in the blood.
Sometimes, when the diuretics do not work (in which case the ascites is said to be refractory), a long needle or catheter is used to draw out the ascitic fluid directly from the abdomen, a procedure called abdominal paracentesis. It is common to withdraw large amounts (liters) of fluid from the abdomen when the ascites is causing painful abdominal distension and/or difficulty breathing because it limits the movement of the diaphragms.
Another treatment for refractory ascites is a procedure called transjugular intravenous portosystemic shunting (TIPS).
The spleen normally acts as a filter to remove older red blood cells, white blood cells, and platelets (small particles important for the clotting of blood). The blood that drains from the spleen joins the blood in the portal vein from the intestines. As the pressure in the portal vein rises in cirrhosis, it increasingly blocks the flow of blood from the spleen. The blood "backs-up," accumulating in the spleen, and the spleen swells in size, a condition referred to as splenomegaly. Sometimes, the spleen is so enlarged it causes abdominal pain.
As the spleen enlarges, it filters out more and more of the blood cells and platelets until their numbers in the blood are reduced. Hypersplenism is the term used to describe this condition, and it is associated with a low red blood cell count (anemia), low white blood cell count (leukopenia), and/or a low platelet count (thrombocytopenia). Anemia can cause weakness, leucopenia can lead to infections, and thrombocytopenia can impair the clotting of blood and result in prolonged bleeding.
 Once varices have bled, they tend to rebleed and the probability that a patient will die from each bleeding episode is high (30% to 35%). Treatment is necessary to prevent the first bleeding episode as well as rebleeding.
Once varices have bled, they tend to rebleed and the probability that a patient will die from each bleeding episode is high (30% to 35%). Treatment is necessary to prevent the first bleeding episode as well as rebleeding. If large varices develop in the esophagus or upper stomach, patients with cirrhosis are at risk for serious bleeding due to rupture of these varices. Once varices have bled, they tend to rebleed and the probability that a patient will die from each bleeding episode is high (30% to 35%). Treatment is necessary to prevent the first bleeding episode as well as rebleeding. Treatments include medications and procedures to decrease the pressure in the portal vein and procedures to destroy the varices.
 Hepatic encephalopathy usually should be treated with a low protein diet and oral lactulose.
Hepatic encephalopathy usually should be treated with a low protein diet and oral lactulose. Patients with an abnormal sleep cycle, impaired thinking, odd behavior, or other signs of hepatic encephalopathy usually should be treated with a low protein diet and oral lactulose. Dietary protein is restricted because it is a source of toxic compounds that cause hepatic encephalopathy. Lactulose, which is a liquid, traps toxic compounds in the colon so they cannot be absorbed into the bloodstream, and thus cause encephalopathy. Lactulose is converted to lactic acid in the colon, and the acidic environment that results is believed to trap the toxic compounds produced by the bacteria. To be sure adequate lactulose is present in the colon at all times, the patient should adjust the dose to produce 2 to 3 semiformed bowel movements a day. Lactulose is a laxative, and the effectiveness of treatment can be judged by loosening or increasing the frequency of stools. Rifaximin (Xifaxan) is an antibiotic taken orally that is not absorbed into the body but rather remains in the intestines. It is the preferred mode of treatment of hepatic encephalopathy. Antibiotics work by suppressing the bacteria that produce the toxic compounds in the colon.
 Most patients with spontaneous bacterial peritonitis are hospitalized and treated with intravenous antibiotics.
Most patients with spontaneous bacterial peritonitis are hospitalized and treated with intravenous antibiotics. Patients suspected of having spontaneous bacterial peritonitis usually will undergo paracentesis. The fluid that is removed is examined for white blood cells and cultured for bacteria. Culturing involves inoculating a sample of the ascites into a bottle of nutrient-rich fluid that encourages the growth of bacteria, thus facilitating the identification of even small numbers of bacteria. Blood and urine samples also are often obtained for culturing because many patients with spontaneous bacterial peritonitis also will have infections in their blood and urine. Many doctors believe the infection may have begun in the blood and the urine and spread to the ascitic fluid to cause spontaneous bacterial peritonitis. Most patients with spontaneous bacterial peritonitis are hospitalized and treated with intravenous antibiotics such as cefotaxime (Claforan). Patients usually treated with antibiotics include:
Spontaneous bacterial peritonitis is a serious infection. It often occurs in patients with advanced cirrhosis whose immune systems are weak, but with modern antibiotics and early detection and treatment, the prognosis of recovering from an episode of spontaneous bacterial peritonitis is good.
In some patients, oral antibiotics (norfloxacin [Noroxin] or sulfamethoxazole and trimethoprim [Bactrim]) can be prescribed to prevent spontaneous bacterial peritonitis. Not all patients with cirrhosis and ascites should be treated with antibiotics to prevent spontaneous bacterial peritonitis, but some patients are at high risk for developing spontaneous bacterial peritonitis and warrant preventive treatment.
 The prognosis and life expectancy for cirrhosis of the liver varies and depends on the cause, the severity, any complications, and any underlying diseases.
The prognosis and life expectancy for cirrhosis of the liver varies and depends on the cause, the severity, any complications, and any underlying diseases. Several types of liver disease that cause cirrhosis (such as hepatitis B and C) are associated with a high incidence of liver cancer. It is useful to screen for liver cancer in patients with cirrhosis, as early surgical treatment or transplantation of the liver can cure the patient of cancer. The difficulty is that the methods available for screening are only partially effective, identifying at best only half of patients at a curable stage of their cancer. Despite the partial effectiveness of screening, most patients with cirrhosis, particularly hepatitis B and C, are screened yearly or every six months with ultrasound examination of the liver and measurements of cancer-produced proteins in the blood, for example, alpha-fetoprotein.
Cirrhosis is irreversible. Liver function usually gradually worsens despite treatment, and complications of cirrhosis increase and become difficult to treat. When cirrhosis is far advanced liver transplantation often is the only option for treatment. Recent advances in surgical transplantation and medications to prevent infection and rejection of the transplanted liver have greatly improved survival after transplantation. On average, more than 80% of patients who receive transplants are alive after five years. Not everyone with cirrhosis is a candidate for transplantation. Furthermore, there is a shortage of livers to transplant, and they're usually is a long (months to years) wait before a liver for transplanting becomes available. Measures to slow the progression of liver disease, and treat and prevent complications of cirrhosis are vitally important.
The prognosis and life expectancy for cirrhosis of the liver varies and depends on the cause, the severity, any complications, and any underlying diseases.
Progress in the management and prevention of cirrhosis continues. Research is ongoing to determine the mechanism of scar formation in the liver and how this process of scarring can be interrupted or even reversed. Newer and better treatments for viral liver disease are being developed to prevent the progression to cirrhosis. Prevention of viral hepatitis by vaccination, which is available for hepatitis B, is being developed for hepatitis C. Treatments for the complications of cirrhosis are being developed or revised, and tested continually. Finally, research is being directed at identifying new proteins in the blood that can detect liver cancer early or predict which patients will develop liver cancer.
 Darmbacterieprofiel kan darmschade voorspellen na radiotherapie
Darmbacterieprofiel kan darmschade voorspellen na radiotherapie
 3 genezingscasestudy's:ben je een moeilijk geval of een mild geval?
3 genezingscasestudy's:ben je een moeilijk geval of een mild geval?
 SCD Met Kip Gevulde Portobello Champignons
SCD Met Kip Gevulde Portobello Champignons
 Wat het betekent om een normale stoelgang te hebben
Wat het betekent om een normale stoelgang te hebben
 De ziekte van Parkinson kan worden voorkomen door darmmicroben
De ziekte van Parkinson kan worden voorkomen door darmmicroben
 Hoe kan ik zure reflux verlichten?
Hoe kan ik zure reflux verlichten?
 Doe mee met The Healthy Gut
Handen omhoog, wie wil helpen een ondersteunende, koesterende en inspirerende gemeenschap vorm te geven, om mensen te ondersteunen bij hun SIBO-reis? Je doet? Dan is dit misschien de perfecte kans voo
Doe mee met The Healthy Gut
Handen omhoog, wie wil helpen een ondersteunende, koesterende en inspirerende gemeenschap vorm te geven, om mensen te ondersteunen bij hun SIBO-reis? Je doet? Dan is dit misschien de perfecte kans voo
 Wat u moet weten over darmreiniging als u PDS heeft
Er is geen tekort aan advertenties die het reinigen van de dubbele punt promoten, waardoor u zich misschien afvraagt of een dubbele puntreiniging veilig is om te proberen voor het prikkelbare darm s
Wat u moet weten over darmreiniging als u PDS heeft
Er is geen tekort aan advertenties die het reinigen van de dubbele punt promoten, waardoor u zich misschien afvraagt of een dubbele puntreiniging veilig is om te proberen voor het prikkelbare darm s
 Wat is een hepaticojejunostomie?
Wat is hepaticojejunostomie? Een hepaticojejunostomie, of Roux-en-Y-procedure, omzeilt de galwegen zodat spijsverteringssappen uit de lever direct in de dunne darm. Het leverkanaal is het buisvorm
Wat is een hepaticojejunostomie?
Wat is hepaticojejunostomie? Een hepaticojejunostomie, of Roux-en-Y-procedure, omzeilt de galwegen zodat spijsverteringssappen uit de lever direct in de dunne darm. Het leverkanaal is het buisvorm