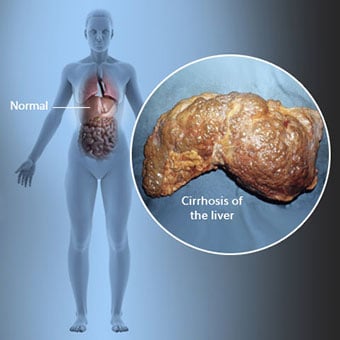
 Цирроз — это осложнение заболевания печени, которое включает потерю клеток печени и необратимое рубцевание печени.
Цирроз — это осложнение заболевания печени, которое включает потерю клеток печени и необратимое рубцевание печени. Лица с циррозом могут иметь мало симптомов и признаков заболевания печени или вообще не иметь их. Некоторые из симптомов могут быть неспецифическими, то есть они не предполагают, что их причиной является печень. Некоторые из наиболее распространенных симптомов и признаков цирроза включают:
У людей с циррозом также появляются симптомы и признаки осложнений цирроза печени.
 Существует множество причин цирроза печени, включая химические вещества (такие как алкоголь, жир и некоторые лекарства), вирусы, токсичные металлы и аутоиммунное заболевание печени, при котором иммунная система организма атакует печень.
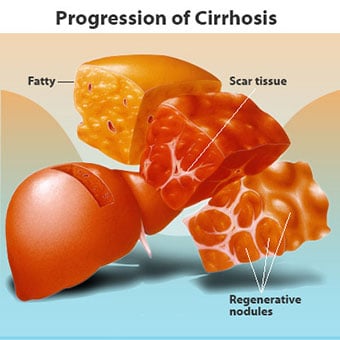
Существует множество причин цирроза печени, включая химические вещества (такие как алкоголь, жир и некоторые лекарства), вирусы, токсичные металлы и аутоиммунное заболевание печени, при котором иммунная система организма атакует печень. Цирроз является осложнением многих заболеваний печени, характеризующихся нарушением структуры и функции печени. Заболевания, которые приводят к циррозу, происходят потому, что они повреждают и убивают клетки печени, после чего воспаление и восстановление, связанные с отмиранием клеток печени, вызывают образование рубцовой ткани. Клетки печени, которые не умирают, размножаются, пытаясь заменить отмершие клетки. Это приводит к скоплению новообразованных клеток печени (регенеративные узелки) в рубцовой ткани. Существует множество причин цирроза, включая химические вещества (такие как алкоголь, жир и некоторые лекарства), вирусы, токсичные металлы (такие как железо и медь, которые накапливаются в печени в результате генетических заболеваний) и аутоиммунные заболевания печени, при которых иммунная система организма атакует печень.
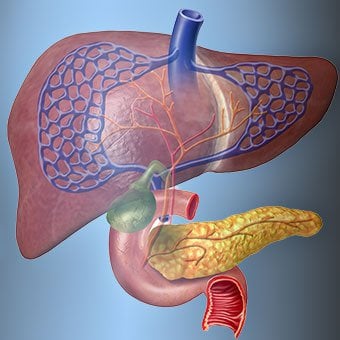
 Связь печени с кровью уникальна.
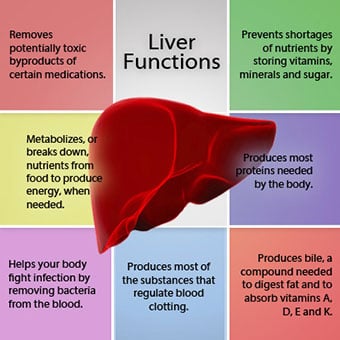
Связь печени с кровью уникальна. Печень является важным органом в организме. Он выполняет множество критических функций, две из которых — производство веществ, необходимых организму, например, свертывание белков, необходимых для свертывания крови, и удаление токсичных веществ, которые могут нанести вред организму, например, таких как лекарства. . Печень также играет важную роль в регулировании поступления глюкозы (сахара) и липидов (жиров), которые организм использует в качестве топлива. Чтобы выполнять эти важные функции, клетки печени должны нормально работать и находиться в непосредственной близости от крови, потому что вещества, добавляемые или удаляемые печенью, транспортируются в печень и из нее кровью.
Связь печени с кровью уникальна. В отличие от большинства органов тела, в печень по артериям поступает лишь небольшое количество крови. Большая часть снабжения печени кровью поступает из кишечных вен, когда кровь возвращается к сердцу. Основная вена, возвращающая кровь из кишечника, называется воротной веной. Когда воротная вена проходит через печень, она распадается на все более мелкие вены. Мельчайшие вены (называемые синусоидами из-за их уникальной структуры) находятся в тесном контакте с клетками печени. Клетки печени выстраиваются вдоль синусоидов. Эта тесная связь между клетками печени и кровью из воротной вены позволяет клеткам печени удалять и добавлять вещества в кровь. Как только кровь проходит через синусоиды, она собирается во все более и более крупные вены, которые в конечном итоге образуют единую печеночную вену, возвращающую кровь к сердцу.
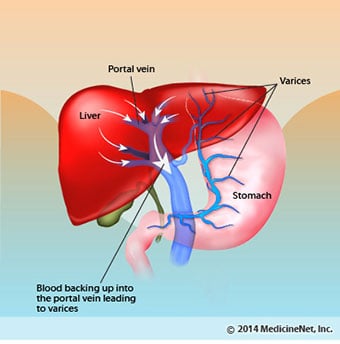
При циррозе нарушается связь между кровью и клетками печени. Несмотря на то, что выжившие или новообразованные клетки печени могут производить и удалять вещества из крови, они не имеют нормальных, близких отношений с кровью, и это препятствует способности клеток печени добавлять или удалять вещества. из крови. Кроме того, рубцевание цирроза печени препятствует току крови через печень и к клеткам печени. В результате препятствия току крови через печень кровь «застаивается» в воротной вене, и давление в воротной вене увеличивается, что называется портальной гипертензией. Из-за обструкции кровотока и высокого давления в воротной вене кровь в воротной вене ищет другие вены, по которым возвращается к сердцу, вены с более низким давлением, которые обходят печень. К сожалению, печень не может добавлять или удалять вещества из крови, которые проходят мимо нее. Это сочетание уменьшенного количества клеток печени, потери нормального контакта между кровью, проходящей через печень, и клетками печени, и кровью, минувшей печень, что приводит ко многим признакам цирроза.
Второй причиной проблем, вызванных циррозом печени, является нарушение взаимоотношений между клетками печени и каналами, по которым течет желчь. Желчь — это жидкость, вырабатываемая клетками печени, которая выполняет две важные функции:помогает пищеварению и выводит из организма токсичные вещества. Желчь, вырабатываемая клетками печени, секретируется в очень крошечные каналы, которые проходят между клетками печени и выстилают синусоиды, называемые канальцами. Канальцы впадают в маленькие протоки, которые затем соединяются, образуя все более и более крупные протоки. Все протоки объединяются в один проток, который входит в тонкую кишку, где помогает перевариванию пищи. При этом токсические вещества, содержащиеся в желчи, попадают в кишечник и затем выводятся с калом. При циррозе канальцы аномальны, и связь между клетками печени и канальцами нарушена, точно так же, как связь между клетками печени и кровью в синусоидах. В результате печень не способна нормально выводить токсические вещества, и они могут накапливаться в организме. В незначительной степени также снижается пищеварение в кишечнике.
 Общие симптомы и признаки цирроза включают желтуху, утомляемость, слабость, потерю аппетита, зуд и легкие кровоподтеки.
Общие симптомы и признаки цирроза включают желтуху, утомляемость, слабость, потерю аппетита, зуд и легкие кровоподтеки. Люди с циррозом могут иметь мало симптомов и признаков заболевания печени или вообще не иметь их. Некоторые из симптомов могут быть неспецифическими и не предполагают, что их причиной является печень. Общие симптомы и признаки цирроза включают:
У людей с циррозом печени также появляются симптомы и признаки осложнений заболевания.
Цирроз сам по себе является уже поздней стадией поражения печени. На ранних стадиях заболевания печени будет воспаление печени. Если это воспаление не лечить, оно может привести к рубцеванию (фиброзу). На этом этапе печень еще может восстановиться при лечении.
Если фиброз печени не лечить, он может привести к циррозу. На этой стадии рубцовая ткань не может зажить, но прогрессирование рубцевания можно предотвратить или замедлить. У людей с циррозом печени, у которых есть признаки осложнений, может развиться терминальная стадия заболевания печени (ESLD), и единственным методом лечения на этой стадии является трансплантация печени.
 Осложнения отеков, асцита и бактериального перитонита
Осложнения отеков, асцита и бактериального перитонита Когда цирроз печени становится тяжелым, в почки посылаются сигналы для удержания соли и воды в организме. Избыток соли и воды сначала накапливается в тканях под кожей лодыжек и ног из-за действия силы тяжести при стоянии или сидении. Это скопление жидкости называется периферическим отеком или точечным отеком. (Точечный отек относится к тому факту, что сильное нажатие кончиком пальца на лодыжку или ногу с отеком вызывает вмятину на коже, которая сохраняется в течение некоторого времени после прекращения давления. Любой тип давления, например, от эластичной ленты носка. , может быть достаточно, чтобы вызвать точечную коррозию.) Отек часто усиливается в конце дня после стояния или сидения и может уменьшаться в течение ночи в положении лежа. По мере ухудшения цирроза печени и удержания большего количества соли и воды жидкость также может скапливаться в брюшной полости между брюшной стенкой и органами брюшной полости (так называемый асцит), вызывая вздутие живота, дискомфорт в животе и увеличение веса.
Жидкость в брюшной полости (асцит) — идеальное место для размножения бактерий. В норме брюшная полость содержит очень небольшое количество жидкости, которая может хорошо сопротивляться инфекции, а бактерии, попадающие в брюшную полость (обычно из кишечника), погибают или попадают в воротную вену и в печень, где погибают. При циррозе жидкость, скапливающаяся в брюшной полости, не может нормально сопротивляться инфекции. Кроме того, больше бактерий попадает из кишечника в асцит. Вероятно возникновение инфекции в брюшной полости и асците, называемой спонтанным бактериальным перитонитом или СБП. СБП является опасным для жизни осложнением. Некоторые пациенты с СБП не имеют симптомов, в то время как у других наблюдается лихорадка, озноб, боль и болезненность в животе, диарея и усиление асцита.
 Кровотечения и осложнения со стороны селезенки
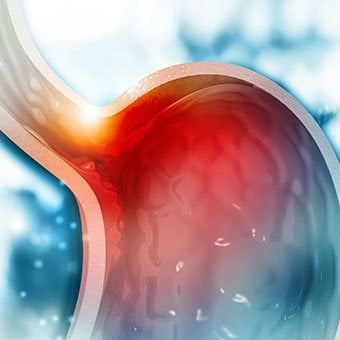
Кровотечения и осложнения со стороны селезенки При циррозе печени рубцовая ткань блокирует поток крови, возвращающейся к сердцу из кишечника, и повышает давление в воротной вене (портальная гипертензия). Когда давление в воротной вене становится достаточно высоким, кровь течет вокруг печени по венам с более низким давлением и достигает сердца. Наиболее распространенными венами, по которым кровь обходит печень, являются вены, выстилающие нижнюю часть пищевода и верхнюю часть желудка.
В результате увеличения притока крови и связанного с этим повышения давления вены в нижних отделах пищевода и верхних отделах желудка расширяются и называются тогда варикозно-расширенными венами пищевода и желудка; чем выше портальное давление, тем больше размер варикозно расширенных вен и тем выше вероятность кровотечения из варикозно расширенных вен в пищевод или желудок.
Кровотечение из варикозно расширенных вен бывает тяжелым и без немедленного лечения может привести к летальному исходу. Симптомы кровотечения из варикозно расширенных вен включают рвоту кровью (она может выглядеть как красная кровь, смешанная со сгустками или «кофейной гущей»), выделение черного и смолистого стула из-за изменений в крови при прохождении через кишечник (мелена) и ортостатический головокружение или обмороки (вызванные падением артериального давления, особенно при вставании из положения лежа).
Кровотечение может редко возникать из варикозно расширенных вен, которые образуются в другом месте кишечника, например, в толстой кишке. Пациенты, госпитализированные по поводу активного кровотечения из варикозно расширенных вен пищевода, имеют высокий риск развития спонтанного бактериального перитонита, хотя причины этого еще не выяснены.
Селезенка обычно действует как фильтр для удаления старых эритроцитов, лейкоцитов и тромбоцитов (мелких частиц, важных для свертывания крови). Кровь, оттекающая от селезенки, присоединяется к крови в воротной вене из кишечника. По мере повышения давления в воротной вене при циррозе она все больше блокирует отток крови от селезенки. Кровь «подпирает», накапливаясь в селезенке, и селезенка увеличивается в размерах, состояние, называемое спленомегалией. Иногда селезенка увеличивается настолько, что вызывает боль в животе.
По мере увеличения селезенки она отфильтровывает все больше и больше клеток крови и тромбоцитов, пока их количество в крови не уменьшится. Гиперспленизм — это термин, используемый для описания этого состояния, и он связан с низким количеством эритроцитов (анемия), низким количеством лейкоцитов (лейкопения) и/или низким количеством тромбоцитов (тромбоцитопения). Анемия может вызвать слабость, лейкопения может привести к инфекциям, а тромбоцитопения может нарушить свертываемость крови и привести к длительному кровотечению
 Осложнения со стороны печени
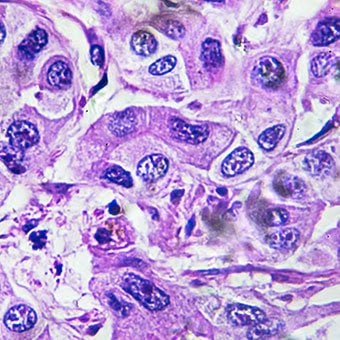
Осложнения со стороны печени Цирроз по любой причине увеличивает риск первичного рака печени (гепатоцеллюлярной карциномы). Первичный относится к тому факту, что опухоль возникает в печени. Вторичный рак печени — это рак, который возникает в другом органе и распространяется (метастазирует) в печень.
Наиболее распространенными симптомами и признаками первичного рака печени являются боль и отек в животе, увеличение печени, потеря веса и лихорадка. Кроме того, рак печени может производить и выделять ряд веществ, в том числе вызывающих увеличение количества эритроцитов (эритроцитоз), низкий уровень сахара в крови (гипогликемия) и высокий уровень кальция в крови (гиперкальциемия).
Некоторая часть белка в пище, которая не переваривается и не всасывается, используется бактериями, обычно присутствующими в кишечнике. При использовании белка в своих целях бактерии производят вещества, которые они выделяют в кишечник, чтобы затем всасываться в организм. Некоторые из этих веществ, например аммиак, могут оказывать токсическое воздействие на мозг. Обычно эти токсичные вещества переносятся из кишечника по воротной вене в печень, где они удаляются из крови и обезвреживаются.
При циррозе клетки печени не могут нормально функционировать либо потому, что они повреждены, либо потому, что они потеряли нормальную связь с кровью. Кроме того, часть крови в воротной вене минует печень по другим венам. Результатом этих нарушений является то, что токсические вещества не могут быть удалены клетками печени, а вместо этого накапливаются в крови.
Когда токсические вещества накапливаются в крови в достаточном количестве, нарушается функция головного мозга, это состояние называется печеночной энцефалопатией. Сон днем, а не ночью (изменение нормального режима сна) является ранним симптомом печеночной энцефалопатии. Другие симптомы включают раздражительность, неспособность концентрироваться или выполнять вычисления, потерю памяти, спутанность сознания или снижение уровня сознания. В конечном итоге тяжелая печеночная энцефалопатия вызывает кому и смерть.
Токсичные вещества также делают мозг пациентов с циррозом очень чувствительным к лекарствам, которые обычно фильтруются и обезвреживаются печенью. Дозы многих лекарств, возможно, придется уменьшить, чтобы избежать накопления токсичности при циррозе печени, особенно седативных средств и препаратов, улучшающих сон. В качестве альтернативы можно использовать препараты, которые не нуждаются в детоксикации или выведении из организма печенью, например препараты, выводимые почками.
У пациентов с ухудшением цирроза печени может развиться гепаторенальный синдром. Этот синдром является тяжелым осложнением, при котором снижается функция почек. Это функциональная проблема в почках, что означает отсутствие физического повреждения почек. Вместо этого сниженная функция связана с изменениями в том, как кровь течет через сами почки. Гепаторенальный синдром определяется как прогрессирующая неспособность почек выводить вещества из крови и вырабатывать достаточное количество мочи при сохранении других важных функций почек, таких как удержание соли. Если функция печени улучшается или больному с гепаторенальным синдромом пересаживают здоровую печень, почки обычно снова начинают нормально работать. Это говорит о том, что снижение функции почек является результатом либо накопления токсических веществ в крови, либо нарушения функции печени при печеночной недостаточности. Различают два типа гепаторенального синдрома. Один тип возникает постепенно в течение нескольких месяцев. Другой происходит быстро в течение недели или двух.
В редких случаях у некоторых пациентов с прогрессирующим циррозом печени может развиться гепатопульмональный синдром. Эти пациенты могут испытывать трудности с дыханием, потому что определенные гормоны, высвобождаемые при прогрессирующем циррозе печени, вызывают ненормальное функционирование легких. Основная проблема в легких заключается в том, что через мелкие кровеносные сосуды в легких, которые соприкасаются с альвеолами (воздушными мешочками) легких, поступает недостаточно крови. Кровь, текущая через легкие, шунтируется вокруг альвеол и не может получить достаточное количество кислорода из воздуха в альвеолах. В результате у пациента возникает одышка, особенно при физической нагрузке.
 Существует 12 распространенных причин цирроза печени.
Существует 12 распространенных причин цирроза печени. Распространенные причины цирроза печени включают:
Менее распространенные причины цирроза включают:
В некоторых частях мира (особенно в Северной Африке) заражение печени паразитами (шистосомоз) является наиболее распространенной причиной заболеваний печени и цирроза.
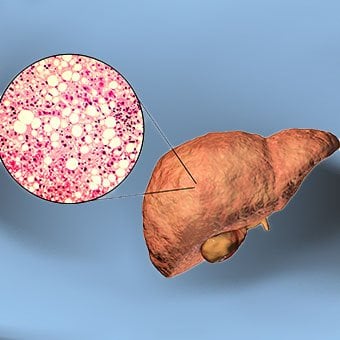 Alcohol and nonalcoholic fatty liver disease are common causes of cirrhosis.
Alcohol and nonalcoholic fatty liver disease are common causes of cirrhosis. Alcohol is a very common cause of cirrhosis, particularly in the Western world. Chronic, high levels of alcohol consumption injure liver cells. Thirty percent of individuals who drink daily at least eight to sixteen ounces of hard liquor or the equivalent for fifteen or more years will develop cirrhosis. Alcohol causes a range of liver diseases, which include simple and uncomplicated fatty liver (steatosis), more serious fatty liver with inflammation (steatohepatitis or alcoholic hepatitis), and cirrhosis.
Nonalcoholic fatty liver disease (NAFLD) refers to a wide spectrum of liver diseases that, like alcoholic liver disease, range from simple steatosis, to nonalcoholic steatohepatitis (NASH), to cirrhosis. All stages of NAFLD have in common the accumulation of fat in liver cells. The term nonalcoholic is used because NAFLD occurs in individuals who do not consume excessive amounts of alcohol, yet in many respects the microscopic picture of NAFLD is similar to what can be seen in liver disease that is due to excessive alcohol. NAFLD is associated with a condition called insulin resistance, which, in turn, is associated with metabolic syndrome and diabetes mellitus type 2. Obesity is the main cause of insulin resistance, metabolic syndrome, and type 2 diabetes. NAFLD is the most common liver disease in the United States and is responsible for up to 25% of all liver disease. The number of livers transplanted for NAFLD-related cirrhosis is on the rise. Public health officials are worried that the current epidemic of obesity will dramatically increase the development of NAFLD and cirrhosis in the population.
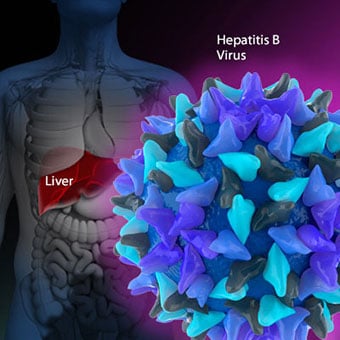 Primary biliary cirrhosis (PBC) is a liver disease caused by an abnormality of the immune system that is found predominantly in women.
Primary biliary cirrhosis (PBC) is a liver disease caused by an abnormality of the immune system that is found predominantly in women. Chronic viral hepatitis is a condition in which hepatitis B or hepatitis C virus infects the liver for years. Most patients with viral hepatitis will not develop chronic hepatitis and cirrhosis. The majority of patients infected with hepatitis A recover completely within weeks, without developing chronic infection. In contrast, some patients infected with hepatitis B virus and most patients infected with hepatitis C virus develop chronic hepatitis, which, in turn, causes progressive liver damage and leads to cirrhosis, and, sometimes, liver cancers.
Autoimmune hepatitis is a liver disease found more commonly in women that is caused by an abnormality of the immune system. The abnormal immune activity in autoimmune hepatitis causes progressive inflammation and destruction of liver cells (hepatocytes), leading ultimately to cirrhosis.
Primary biliary cirrhosis (PBC) is a liver disease caused by an abnormality of the immune system that is found predominantly in women. The abnormal immunity in PBC causes chronic inflammation and destruction of the small bile ducts within the liver. The bile ducts are passages within the liver through which bile travels to the intestine. Bile is a fluid produced by the liver that contains substances required for digestion and absorption of fat in the intestine, as well as other compounds that are waste products, such as the pigment bilirubin. (Bilirubin is produced by the breakdown of hemoglobin from old red blood cells.). Along with the gallbladder, the bile ducts make up the biliary tract. In PBC, the destruction of the small bile ducts blocks the normal flow of bile into the intestine. As the inflammation continues to destroy more of the bile ducts, it also spreads to destroy nearby liver cells. As the destruction of the hepatocytes proceeds, scar tissue (fibrosis) forms and spreads throughout the areas of destruction. The combined effects of progressive inflammation, scarring, and the toxic effects of accumulating waste products culminates in cirrhosis.
Primary sclerosing cholangitis (PSC) is an uncommon disease frequently found in patients with Crohn's disease and ulcerative colitis. In PSC, the large bile ducts outside of the liver become inflamed, narrowed, and obstructed. Obstruction to the flow of bile leads to infections of the bile ducts and jaundice, eventually causing cirrhosis. In some patients, injury to the bile ducts (usually because of surgery) also can cause obstruction and cirrhosis of the liver.
 Different liver diseases should be diagnosed by specialists and different tests such as liver blood test, biopsy, and others.
Different liver diseases should be diagnosed by specialists and different tests such as liver blood test, biopsy, and others. Inherited (genetic) disorders that result in the accumulation of toxic substances in the liver, which leads to tissue damage and cirrhosis. Examples include the abnormal accumulation of iron (hemochromatosis) or copper (Wilson disease). In hemochromatosis, patients inherit a tendency to absorb an excessive amount of iron from food. Over time, iron accumulation in different organs throughout the body causes cirrhosis, arthritis, heart muscle damage leading to heart failure, and testicular dysfunction causing loss of sexual drive. Treatment is aimed at preventing damage to organs by removing iron from the body through phlebotomy (removing blood). In Wilson disease, there is an inherited abnormality in one of the proteins that control copper in the body. Over time, copper accumulates in the liver, eyes, and brain. Cirrhosis, tremor, psychiatric disturbances, and other neurological difficulties occur if the condition is not treated early. Treatment is with oral medication, which increases the amount of copper that is eliminated from the body in the urine.
Cryptogenic cirrhosis (cirrhosis due to unidentified causes) is a common reason for liver transplantation. It is termed called cryptogenic cirrhosis because for many years doctors have been being unable to explain why a proportion of patients developed cirrhosis. Doctors now believe that cryptogenic cirrhosis is due to NASH (nonalcoholic steatohepatitis) caused by long-standing obesity, type 2 diabetes, and insulin resistance. The fat in the liver of patients with NASH is believed to disappear with the onset of cirrhosis, and this has made it difficult for doctors to make the connection between NASH and cryptogenic cirrhosis for a long time. One important clue that NASH leads to cryptogenic cirrhosis is the finding of a high occurrence of NASH in the new livers of patients undergoing liver transplant for cryptogenic cirrhosis. Finally, a study from France suggests that patients with NASH have a similar risk of developing cirrhosis as patients with long-standing infection with hepatitis C virus. (See discussion that follows.) However, the progression to cirrhosis from NASH is thought to be slow and the diagnosis of cirrhosis typically is made in people in their sixties.
Infants can be born without bile ducts (biliary atresia) and ultimately develop cirrhosis. Other infants are born lacking vital enzymes for controlling sugars that lead to the accumulation of sugars and cirrhosis. On rare occasions, the absence of a specific enzyme can cause cirrhosis and scarring of the lung (alpha-1 antitrypsin deficiency).
Less common causes of cirrhosis include unusual reactions to some drugs and prolonged exposure to toxins, as well as chronic heart failure (cardiac cirrhosis). In certain parts of the world (particularly Northern Africa), infection of the liver with a parasite (schistosomiasis) is the most common cause of liver disease and cirrhosis.
Different liver diseases should be diagnosed by specialists and different tests such as liver blood test, biopsy, and others. The single best test for diagnosing cirrhosis is a biopsy of the liver. Liver biopsies carry a small risk for serious complications, and biopsy often is reserved for those patients in whom the diagnosis of the type of liver disease or the presence of cirrhosis is not clear. The history, physical examination, or routine testing may suggest the possibility of cirrhosis. If cirrhosis is present, other tests can be used to determine the severity of the cirrhosis and the presence of complications. Tests also may be used to diagnose the underlying disease that is causing the cirrhosis. Examples of how doctors diagnose and evaluate cirrhosis are:
 There are four types of treatment of cirrhosis.
There are four types of treatment of cirrhosis. Treatment of cirrhosis includes
Consume a balanced diet and one multivitamin daily. Patients with PBC with impaired absorption of fat-soluble vitamins may need additional vitamins D and K.
Avoid drugs (including alcohol) that cause liver damage. All patients with cirrhosis should avoid alcohol. Most patients with alcohol-induced cirrhosis experience an improvement in liver function with abstinence from alcohol. Even patients with chronic hepatitis B and C can substantially reduce liver damage and slow the progression towards cirrhosis with abstinence from alcohol.
Avoid nonsteroidal anti-inflammatory drugs (NSAIDs, e.g., ibuprofen). Patients with cirrhosis can experience worsening of liver and kidney function with NSAIDs.
Eradicate hepatitis B and hepatitis C virus by using anti-viral medications. Not all patients with cirrhosis due to chronic viral hepatitis are candidates for drug treatment. Some patients may experience serious deterioration in liver function and/or intolerable side effects during treatment. Thus, decisions to treat viral hepatitis have to be individualized, after consulting with doctors experienced in treating liver diseases (hepatologists).
Remove blood from patients with hemochromatosis to reduce the levels of iron and prevent further damage to the liver. In Wilson's disease, medications can be used to increase the excretion of copper in the urine to reduce the levels of copper in the body and prevent further damage to the liver.
Suppress the immune system with drugs such as prednisone and azathioprine (Imuran) to decrease inflammation of the liver in autoimmune hepatitis.
Treat patients with PBC with a bile acid preparation, ursodeoxycholic acid (UDCA), also called ursodiol (Actigall). Results of an analysis that combined the results from several clinical trials showed that UDCA increased survival among PBC patients during 4 years of therapy. The development of portal hypertension also was reduced by the UDCA. It is important to note that despite producing clear benefits, UDCA treatment primarily retards progression and does not cure PBC. Other medications such as colchicine and methotrexate also may have benefits in subsets of patients with PBC.
Immunize patients with cirrhosis against infection with hepatitis A and B to prevent a serious deterioration in liver. There are currently no vaccines available for immunizing against hepatitis C.
 Treatment for edema, ascites, and hypersplenism complications.
Treatment for edema, ascites, and hypersplenism complications. Retaining salt and water can lead to swelling of the ankles and legs (edema) or abdomen (ascites) in patients with cirrhosis. Doctors often advise patients with cirrhosis to restrict dietary salt (sodium) and fluid to decrease edema and ascites. The amount of salt in the diet usually is restricted to 2 grams per day and fluid to 1.2 liters per day. In most patients with cirrhosis, salt and fluid restriction is not enough and diuretics have to be added.
Diuretics are medications that work in the kidneys to promote the elimination of salt and water into the urine. A combination of the diuretics spironolactone (Aldactone) and furosemide (Lasix) can reduce or eliminate the edema and ascites in most patients. During treatment with diuretics, it is important to monitor the function of the kidneys by measuring blood levels of blood urea nitrogen (BUN) and creatinine to determine if too much diuretic is being used. Too much diuretic can lead to kidney dysfunction that is reflected in elevations of the BUN and creatinine levels in the blood.
Sometimes, when the diuretics do not work (in which case the ascites is said to be refractory), a long needle or catheter is used to draw out the ascitic fluid directly from the abdomen, a procedure called abdominal paracentesis. It is common to withdraw large amounts (liters) of fluid from the abdomen when the ascites is causing painful abdominal distension and/or difficulty breathing because it limits the movement of the diaphragms.
Another treatment for refractory ascites is a procedure called transjugular intravenous portosystemic shunting (TIPS).
The spleen normally acts as a filter to remove older red blood cells, white blood cells, and platelets (small particles important for the clotting of blood). The blood that drains from the spleen joins the blood in the portal vein from the intestines. As the pressure in the portal vein rises in cirrhosis, it increasingly blocks the flow of blood from the spleen. The blood "backs-up," accumulating in the spleen, and the spleen swells in size, a condition referred to as splenomegaly. Sometimes, the spleen is so enlarged it causes abdominal pain.
As the spleen enlarges, it filters out more and more of the blood cells and platelets until their numbers in the blood are reduced. Hypersplenism is the term used to describe this condition, and it is associated with a low red blood cell count (anemia), low white blood cell count (leukopenia), and/or a low platelet count (thrombocytopenia). Anemia can cause weakness, leucopenia can lead to infections, and thrombocytopenia can impair the clotting of blood and result in prolonged bleeding.
 Once varices have bled, they tend to rebleed and the probability that a patient will die from each bleeding episode is high (30% to 35%). Treatment is necessary to prevent the first bleeding episode as well as rebleeding.
Once varices have bled, they tend to rebleed and the probability that a patient will die from each bleeding episode is high (30% to 35%). Treatment is necessary to prevent the first bleeding episode as well as rebleeding. If large varices develop in the esophagus or upper stomach, patients with cirrhosis are at risk for serious bleeding due to rupture of these varices. Once varices have bled, they tend to rebleed and the probability that a patient will die from each bleeding episode is high (30% to 35%). Treatment is necessary to prevent the first bleeding episode as well as rebleeding. Treatments include medications and procedures to decrease the pressure in the portal vein and procedures to destroy the varices.
 Hepatic encephalopathy usually should be treated with a low protein diet and oral lactulose.
Hepatic encephalopathy usually should be treated with a low protein diet and oral lactulose. Patients with an abnormal sleep cycle, impaired thinking, odd behavior, or other signs of hepatic encephalopathy usually should be treated with a low protein diet and oral lactulose. Dietary protein is restricted because it is a source of toxic compounds that cause hepatic encephalopathy. Lactulose, which is a liquid, traps toxic compounds in the colon so they cannot be absorbed into the bloodstream, and thus cause encephalopathy. Lactulose is converted to lactic acid in the colon, and the acidic environment that results is believed to trap the toxic compounds produced by the bacteria. To be sure adequate lactulose is present in the colon at all times, the patient should adjust the dose to produce 2 to 3 semiformed bowel movements a day. Lactulose is a laxative, and the effectiveness of treatment can be judged by loosening or increasing the frequency of stools. Rifaximin (Xifaxan) is an antibiotic taken orally that is not absorbed into the body but rather remains in the intestines. It is the preferred mode of treatment of hepatic encephalopathy. Antibiotics work by suppressing the bacteria that produce the toxic compounds in the colon.
 Most patients with spontaneous bacterial peritonitis are hospitalized and treated with intravenous antibiotics.
Most patients with spontaneous bacterial peritonitis are hospitalized and treated with intravenous antibiotics. Patients suspected of having spontaneous bacterial peritonitis usually will undergo paracentesis. The fluid that is removed is examined for white blood cells and cultured for bacteria. Culturing involves inoculating a sample of the ascites into a bottle of nutrient-rich fluid that encourages the growth of bacteria, thus facilitating the identification of even small numbers of bacteria. Blood and urine samples also are often obtained for culturing because many patients with spontaneous bacterial peritonitis also will have infections in their blood and urine. Many doctors believe the infection may have begun in the blood and the urine and spread to the ascitic fluid to cause spontaneous bacterial peritonitis. Most patients with spontaneous bacterial peritonitis are hospitalized and treated with intravenous antibiotics such as cefotaxime (Claforan). Patients usually treated with antibiotics include:
Spontaneous bacterial peritonitis is a serious infection. It often occurs in patients with advanced cirrhosis whose immune systems are weak, but with modern antibiotics and early detection and treatment, the prognosis of recovering from an episode of spontaneous bacterial peritonitis is good.
In some patients, oral antibiotics (norfloxacin [Noroxin] or sulfamethoxazole and trimethoprim [Bactrim]) can be prescribed to prevent spontaneous bacterial peritonitis. Not all patients with cirrhosis and ascites should be treated with antibiotics to prevent spontaneous bacterial peritonitis, but some patients are at high risk for developing spontaneous bacterial peritonitis and warrant preventive treatment.
 The prognosis and life expectancy for cirrhosis of the liver varies and depends on the cause, the severity, any complications, and any underlying diseases.
The prognosis and life expectancy for cirrhosis of the liver varies and depends on the cause, the severity, any complications, and any underlying diseases. Several types of liver disease that cause cirrhosis (such as hepatitis B and C) are associated with a high incidence of liver cancer. It is useful to screen for liver cancer in patients with cirrhosis, as early surgical treatment or transplantation of the liver can cure the patient of cancer. The difficulty is that the methods available for screening are only partially effective, identifying at best only half of patients at a curable stage of their cancer. Despite the partial effectiveness of screening, most patients with cirrhosis, particularly hepatitis B and C, are screened yearly or every six months with ultrasound examination of the liver and measurements of cancer-produced proteins in the blood, for example, alpha-fetoprotein.
Cirrhosis is irreversible. Liver function usually gradually worsens despite treatment, and complications of cirrhosis increase and become difficult to treat. When cirrhosis is far advanced liver transplantation often is the only option for treatment. Recent advances in surgical transplantation and medications to prevent infection and rejection of the transplanted liver have greatly improved survival after transplantation. On average, more than 80% of patients who receive transplants are alive after five years. Not everyone with cirrhosis is a candidate for transplantation. Furthermore, there is a shortage of livers to transplant, and they're usually is a long (months to years) wait before a liver for transplanting becomes available. Measures to slow the progression of liver disease, and treat and prevent complications of cirrhosis are vitally important.
The prognosis and life expectancy for cirrhosis of the liver varies and depends on the cause, the severity, any complications, and any underlying diseases.
Progress in the management and prevention of cirrhosis continues. Research is ongoing to determine the mechanism of scar formation in the liver and how this process of scarring can be interrupted or even reversed. Newer and better treatments for viral liver disease are being developed to prevent the progression to cirrhosis. Prevention of viral hepatitis by vaccination, which is available for hepatitis B, is being developed for hepatitis C. Treatments for the complications of cirrhosis are being developed or revised, and tested continually. Finally, research is being directed at identifying new proteins in the blood that can detect liver cancer early or predict which patients will develop liver cancer.
 Безопасен ли арахис при СРК? Развенчание мифов об афлатоксинах.
Безопасен ли арахис при СРК? Развенчание мифов об афлатоксинах.
 Как избавиться от геморроя:виды, причины и лечение
Как избавиться от геморроя:виды, причины и лечение
 Пеммикан с беконом — идеальная палеодиета для путешествий
Пеммикан с беконом — идеальная палеодиета для путешествий
 Каковы типы разрезов брюшной полости?
Каковы типы разрезов брюшной полости?
 Победить Summer Bloat
Победить Summer Bloat
 Желудочный грипп (гастроэнтерит) Симптомы Признаки, лечение Средства, диета
Желудочный грипп (гастроэнтерит) Симптомы Признаки, лечение Средства, диета
 Что такое анализ крови на АЛТ? Признаки поражения печени
Тест на АЛТ (аланинтрансаминазу) измеряет уровень АЛТ в крови для выявления повреждений или заболеваний печени. Тест на АЛТ (аланинтрансаминазу) измеряет уровень АЛТ в крови для выявления повреждений
Что такое анализ крови на АЛТ? Признаки поражения печени
Тест на АЛТ (аланинтрансаминазу) измеряет уровень АЛТ в крови для выявления повреждений или заболеваний печени. Тест на АЛТ (аланинтрансаминазу) измеряет уровень АЛТ в крови для выявления повреждений
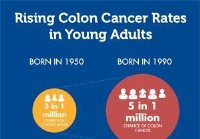 Новый возраст начала скрининга рака толстой кишки
Американское онкологическое общество (ACS) недавно обновило свои рекомендации по возрасту начала скрининга рака толстой кишки, чтобы теперь они начинались с 45 лет для людей со средним риском. Это важ
Новый возраст начала скрининга рака толстой кишки
Американское онкологическое общество (ACS) недавно обновило свои рекомендации по возрасту начала скрининга рака толстой кишки, чтобы теперь они начинались с 45 лет для людей со средним риском. Это важ
 SCD Spaghetti (забудьте о лапше, главное — это соус)
В детстве мы ездили на машине из Мичигана во Флориду, и я заказывал спагетти на каждый прием пищи туда и обратно. Я также попросила маму приготовить мне свои знаменитые спагетти 10 лет подряд на мой д
SCD Spaghetti (забудьте о лапше, главное — это соус)
В детстве мы ездили на машине из Мичигана во Флориду, и я заказывал спагетти на каждый прием пищи туда и обратно. Я также попросила маму приготовить мне свои знаменитые спагетти 10 лет подряд на мой д