 ¿Qué es el VHC, cómo se transmite, hay síntomas y es curable?
¿Qué es el VHC, cómo se transmite, hay síntomas y es curable?La mayoría de las personas que contraen hepatitis C (hep C) no tienen síntomas. Sin embargo, aquellos que sí tienen síntomas pueden experimentar:
La infección por el virus de la hepatitis C es una infección del hígado causada por el virus de la hepatitis C (también conocido como VHC o hepatitis C). Es difícil para el sistema inmunitario humano eliminar la hepatitis C del cuerpo, y la infección por hepatitis C generalmente se vuelve crónica. Durante décadas, la infección crónica por hepatitis C daña el hígado y puede causar insuficiencia hepática. En los EE. UU., los CDC han estimado que se produjeron aproximadamente 41 200 nuevos casos de hepatitis C en 2016. Cuando el virus ingresa por primera vez al cuerpo, generalmente no hay síntomas, por lo que este número es una estimación. Alrededor del 75% al 85% de las personas recién infectadas se infectan crónicamente. En los EE. UU., se estima que más de 2 millones de personas están crónicamente infectadas con hepatitis C. La infección se detecta con mayor frecuencia entre las personas de 40 a 60 años de edad, lo que refleja las altas tasas de infección en las décadas de 1970 y 1980. Hay entre 8000 y 10 000 muertes cada año en los EE. UU. relacionadas con la infección por hepatitis C. La infección por VHC es la principal causa de trasplante de hígado en los EE. UU. y es un factor de riesgo para el cáncer de hígado. En 2016, 18 153 certificados de defunción enumeraron el VHC como una causa contribuyente de muerte; se cree que esto es una subestimación.
Alrededor del 10% al 20% de las personas que desarrollan VHC crónica desarrollarán cirrosis dentro de 20 a 30 años. La progresión a la cirrosis puede acelerarse con más de 50 años, sexo masculino, consumo de alcohol, enfermedad del hígado graso no alcohólico (EHNA), coinfección con hepatitis B o VIH y fármacos inmunosupresores. La infección por VHC es la principal causa de trasplante de hígado debido a insuficiencia hepática en los EE. UU.
Aquellos que tienen cirrosis por VHC también tienen un riesgo anual de cáncer de hígado (hepatoma o carcinoma hepatocelular) de alrededor del 1% al 5%.
Hepatitis significa inflamación del hígado. La hepatitis C es uno de varios virus que pueden causar hepatitis viral. No está relacionado con los otros virus comunes de la hepatitis (por ejemplo, hepatitis A o hepatitis B). La hepatitis C es un miembro de la Flaviviridae familia de virus. Otros miembros de esta familia de virus incluyen los que causan la fiebre amarilla y el dengue.
Hay al menos seis genotipos (cepas) diferentes del virus que tienen diferentes perfiles genéticos (genotipos 1 a 6). En los EE. UU., el genotipo 1 es la cepa más común de la hepatitis C. Incluso dentro de un solo genotipo puede haber algunas variaciones (genotipo 1a y 1b, por ejemplo). La genotipificación se usa para guiar el tratamiento porque algunos genotipos virales responden mejor a algunas terapias que a otras.
Al igual que el virus de la inmunodeficiencia humana (VIH), la hepatitis C se multiplica muy rápido y alcanza niveles muy altos en el organismo. Los genes que hacen que las proteínas de la superficie del virus también muten (cambien) rápidamente, y diariamente se producen miles de variaciones genéticas del virus ("cuasi-especies"). Es imposible que el cuerpo siga produciendo anticuerpos anti-VHC contra todas las cuasi-especies que circulan al mismo tiempo. Todavía no ha sido posible desarrollar una vacuna efectiva porque la vacuna debe proteger contra todos los genotipos.
La infección por hepatitis C en el hígado activa el sistema inmunitario, lo que conduce a la inflamación. Alrededor del 20% al 30% de las personas con infección aguda experimentarán los síntomas típicos de la hepatitis, como dolor abdominal, ictericia, orina oscura o heces de color arcilla. Sin embargo, la hepatitis C crónica por lo general no causa síntomas hasta muy avanzada la enfermedad, y los pacientes se refieren a la hepatitis C como el "dragón dormido". Durante varios años o décadas, la inflamación crónica puede causar la muerte de las células hepáticas y la formación de cicatrices ("fibrosis"). La cicatrización extensa en el hígado se llama cirrosis. Esto deteriora progresivamente las funciones vitales del hígado. Los hígados cirróticos son más propensos al cáncer de hígado. Beber alcohol acelera el daño hepático con la hepatitis C. La infección por VIH concurrente, así como la infección aguda por hepatitis A o B, también acelerará la progresión a la cirrosis.
Alrededor del 70% al 80% de las personas no tienen síntomas cuando se infectan por primera vez con el VHC. El 20%-30% restante puede tener
Los primeros síntomas de la hepatitis C pueden incluir orina oscura, ojos amarillos o heces de color arcilla, aunque esto es inusual. Con el tiempo, las personas con infección crónica por VHC pueden desarrollar signos de inflamación hepática que sugieran que la infección puede estar presente. Las personas infectadas pueden fatigarse con facilidad o quejarse de síntomas inespecíficos. Los últimos síntomas y signos de cirrosis suelen estar ausentes hasta que la inflamación está bastante avanzada. A medida que avanza la cirrosis, los síntomas y signos aumentan y pueden incluir:
Debido a que la hepatitis C se transmite por exposición a la sangre, no existe un período específico de contagio. Las personas que desarrollan hepatitis C crónica portan el virus en la sangre y, por lo tanto, son contagiosas para los demás durante toda su vida, a menos que se curen de la hepatitis C.
Es difícil decir con certeza cuál es el período de incubación de la hepatitis C, porque la mayoría de las personas que están infectadas con hepatitis C no tienen síntomas al principio del curso de la infección. Aquellos que desarrollan síntomas temprano después de infectarse (de 2 a 12 semanas en promedio, pero puede ser más) experimentan síntomas gastrointestinales leves que pueden no provocar una visita al médico.
La mayoría de los signos y síntomas de la infección por hepatitis C se relacionan con el hígado. Con menos frecuencia, la infección por hepatitis C puede afectar otros órganos además del hígado.
La infección por hepatitis C puede hacer que el cuerpo produzca anticuerpos anormales llamados crioglobulinas. Las crioglobulinas causan inflamación de las arterias (vasculitis). Esto puede dañar la piel, las articulaciones y los riñones. Los pacientes con crioglobulinemia (crioglobulinas en la sangre) pueden tener
Además, las personas infectadas con crioglobulinemia pueden desarrollar el fenómeno de Raynaud en el que los dedos de las manos y de los pies se vuelven de color (blanco, luego morado, luego rojo) y se vuelven dolorosos a bajas temperaturas.
El grupo de trabajo de los Servicios de Salud Preventiva de EE. UU. recomienda que todos los adultos nacidos entre 1945 y 1965 se hagan una prueba de rutina para la hepatitis C, independientemente de si existen factores de riesgo para la hepatitis C. También se recomienda una prueba única para:
Las personas que pueden haber estado expuestas a la hepatitis C en los 6 meses anteriores deben someterse a una prueba de carga de ARN viral en lugar de anticuerpos contra el VHC, ya que es posible que los anticuerpos no estén presentes hasta 12 semanas o más después de la infección, aunque el ARN del VHC puede ser detectable. en sangre tan pronto como 2-3 semanas después de la infección.
En general, la evaluación anual puede ser apropiada para personas con factores de riesgo continuos, como enfermedades de transmisión sexual (ETS) repetidas o muchas parejas sexuales, uso continuo de drogas por vía intravenosa o parejas sexuales a largo plazo de personas con hepatitis C. estas personas se determina en una decisión caso por caso.
Existe un riesgo del 4% al 7% de transmitir el VHC de madre a hijo con cada embarazo. Actualmente, no existe una recomendación de los CDC para la detección de rutina de la hepatitis C durante el embarazo, y actualmente no existe un medicamento recomendado para prevenir la transmisión de madre a hijo (profilaxis). Sin embargo, los CDC están monitoreando los hallazgos de la investigación y pueden hacer recomendaciones en el futuro a medida que surja la evidencia.
Si bien los datos aún son limitados, un estudio reciente de más de 1000 casos en el Reino Unido encontró que el 11 % de los bebés habían sido infectados al nacer y que era probable que estos bebés desarrollaran cirrosis a los 30 años. El caso de la detección del VHC durante el embarazo incluye la posibilidad de tratar de manera segura a las madres durante el embarazo con agentes antivirales de acción directa (AAD) para tratar a la madre antes de que se desarrolle la cirrosis, prevenir la transmisión infantil y prevenir la transmisión a otros. A los niños nacidos de madres infectadas con el VHC también se les puede ofrecer tratamiento a una edad temprana para prevenir la cirrosis, así como la transmisión a otros. La coordinación de la atención entre varios especialistas será importante para lograr estos objetivos.
Los niños de madres infectadas con el VHC pueden someterse a pruebas de detección de hepatitis C a los 1 o 2 meses de edad mediante pruebas de PCR o carga viral de hepatitis C (consulte Análisis de sangre para la hepatitis C). Los anticuerpos contra la hepatitis C que se transmiten de madre a hijo estarán presentes hasta por 18 meses, por lo que los niños no deben someterse a pruebas de detección de anticuerpos contra el VHC antes.
La hepatitis C es tratada por un gastroenterólogo, un hepatólogo (un gastroenterólogo con capacitación adicional en enfermedades hepáticas) o un especialista en enfermedades infecciosas. El equipo de tratamiento puede incluir más de un especialista, según la extensión del daño hepático. Los cirujanos que se especializan en cirugía del hígado, incluido el trasplante de hígado, forman parte del equipo médico y deben atender a pacientes con enfermedad avanzada (insuficiencia hepática o cirrosis) temprano, antes de que el paciente necesite un trasplante de hígado. Es posible que puedan identificar los problemas que deben abordarse antes de que se pueda considerar la cirugía. Otras personas que pueden ser útiles en el manejo de pacientes incluyen dietistas para consultar sobre temas nutricionales y farmacéuticos para ayudar con el manejo de medicamentos.
Existen varios análisis de sangre para el diagnóstico de la infección por hepatitis C. La sangre se puede analizar para detectar anticuerpos contra la hepatitis C (anticuerpos anti-VHC). Los anticuerpos tardan entre 8 y 12 semanas en promedio y hasta 6 meses en desarrollarse después de la infección inicial con hepatitis C, por lo que la detección de anticuerpos puede pasar por alto a algunas personas recién infectadas. Tener anticuerpos no es una indicación absoluta de que el virus de la hepatitis C se multiplica y está activo, pero si la prueba de anticuerpos es positiva (el anticuerpo está presente), la probabilidad estadística de infección activa es superior al 99 %.
Hay varias pruebas disponibles para medir la cantidad de virus de la hepatitis C en la sangre de una persona (la carga viral). El ARN del virus de la hepatitis C puede identificarse mediante un tipo de prueba llamada reacción en cadena de la polimerasa (PCR) que detecta el virus circulante en la sangre tan pronto como 2 o 3 semanas después de la infección, por lo que puede usarse para detectar sospechas de infección aguda por hepatitis C. infección temprana. También se usa para determinar si alguien que tiene anticuerpos contra la hepatitis C tiene hepatitis activa y para hacer un seguimiento de la carga viral durante el tratamiento.
También se realizan análisis de sangre para identificar los genotipos del VHC. Los genotipos responden de manera diferente a diferentes tratamientos, por lo que esta información es importante en la selección del régimen de tratamiento más apropiado.
La estimación de la fibrosis hepática mediante análisis de sangre también es bastante confiable para diagnosticar cicatrices clínicamente significativas; estos incluyen FIB-4, FibroSure, Fibrotest y el índice de proporción de aspartato aminotransferasa a plaquetas (APRI).
El siguiente paso es determinar el nivel de cicatrización hepática que se ha producido. La biopsia de hígado permite el examen de una pequeña muestra de tejido hepático bajo un microscopio, sin embargo, la biopsia de hígado es una prueba invasiva y tiene riesgos significativos de sangrado. También podría pasar por alto áreas anormales en las primeras etapas de la enfermedad.
Las pruebas no invasivas han reemplazado en gran medida a la biopsia hepática, excepto en situaciones especiales. La rigidez del hígado indica que puede haber cirrosis o cicatrización avanzada del hígado. La elastografía transitoria se puede usar para medir esta rigidez mediante ultrasonido o resonancia magnética nuclear (RMN).
La evaluación previa al tratamiento para la hepatitis C también debe incluir:
Interferons, for example, Roferon-A and Infergen, and pegylated interferons such as Peg-Intron T , Pegasys, were mainstays of treatment for years. Interferons produced sustained viral response (SVR, or cure) of up to 15%. Later, peglatedll forms produced SVR of 50%-80%. These drugs were injected, had many adverse effects, required frequent monitoring, and were often combined with oral ribavirin, which caused anemia. Treatment durations ranged up to 48 weeks.
Direct-acting anti-viral agents (DAAs) are antiviral drugs that act directly on hepatitis C multiplication.
Hepatitis C treatment is best discussed with a doctor or specialist familiar with current and developing options as this field is changing, and even major guidelines may become outdated quickly.
The latest treatment guidelines by the American Association for the Study of Liver Disease (AASLD) and Infectious Disease Society of America (IDSA) recommends use of DAAs as first-line treatment for hepatitis C infection. The choice of DAA varies by specific virus genotype, and the presence or absence of cirrhosis. In the U.S., specific insurance providers also might influence the choice due to the high cost of DAAs. Although the individual, public health, and cost benefits of treating all patients with hepatitis C is clear, the most difficult barrier to treating all people with HCV is the very high cost of the drug regimens. Patients are encouraged to discuss options with their health care professional.
Treatment is recommended in all patients with chronic hepatitis C unless they have a short life expectancy that is not related to liver disease. Severe life-threatening liver disease may require liver transplantation. Newer therapies with DAAs have allowed more and more patients to be treated.
The ultimate goals of antiviral therapy are to
A side goal is preventing co-infections with other hepatitis viruses, such as A and B, which can cause more liver disease than HCV alone. These can be prevented by vaccines and treatment.
When people first get hepatitis C, the infection is said to be acute. Most people with acute hepatitis C do not have symptoms so they are not recognized as being infected. However, some have low-grade fever, fatigue or other symptoms that lead to an early diagnosis. Others who become infected and have a known exposure to an infected source, such as a needlestick injury, are monitored closely.
Treatment decisions should be made on a case-by-case basis. Response to treatment is higher in acute hepatitis infection than chronic infection. However, many experts prefer to hold off treatment for 8-12 weeks to see whether the patient naturally eliminates the virus without treatment. Approaches to treatment are evolving. Patients with acute hepatitis C infection should discuss treatment options with a health care professional who is experienced in treating the disease. There is no established treatment regimen at this time.
If the hepatitis C RNA remains undetectable at the end of the treatment and follow-up period, this is called a sustained virologic response (SVR) and is considered a cure. Over 90% of people treated with DAAs are cured. These people have significantly reduced liver inflammation, and liver scarring may even be reversed.
About 5% of people who are treated for HCV infection are not cured by some of the older regimens. These people may still have options for cure with the newer regimens.
Few people with hepatitis C are at risk for problems if they are treated, however there are some factors that affect treatment regimens, such as concurrent HIV medications and kidney dysfunction. Some drugs are not safe for people with cirrhosis. Individuals who are unable to comply with the treatment schedule for psychological reasons or ongoing drug or alcohol abuse may not be good candidates for treatment because the drugs are very costly and require adherence to the pill regimen and regular follow-up visits. There are some important drug interactions with some of the medications that should be considered by the health care professional.
People with past hepatitis B or who have chronic active hepatitis B should not be treated for HCV without treating for HBV as well. As highly effective treatment for HCV has emerged, reports of serious hepatitis B have come to light. Similar to HCV, hepatitis B usually does not clear from the liver after acute infection, even though it is far less likely to cause chronic active hepatitis than hepatitis C infection. It remains dormant in most people, but it can reactivate with changes in the immune system. It is not clear why eliminating the HCV can allow the HBV infection to flare up. Hepatitis B screening is an important part of the hepatitis C evaluation. Those who have laboratory evidence of active or past infection with HBV should be monitored while receiving HCV treatment.
Compared to interferons and ribavirin drugs, the side effects of DAAs are far fewer and more tolerable. These side effects usually do not require discontinuation of therapy and are self-limiting after completion of therapy.
Patients with hepatitis B co-infection should be monitored for symptoms of reactivation of hepatitis, which are the same as the symptoms of acute hepatitis. The treating doctor may perform blood screening for this as well.
Hepatitis C is the leading reason for 40% to 45% of liver transplants in the U.S. Hepatitis C usually recurs after transplantation and infects the new liver. Approximately 25% of these patients with recurrent hepatitis will develop cirrhosis within five years of transplantation. Despite this, the five-year survival rate for patients with hepatitis C is similar to that of patients who are transplanted for other types of liver disease.
Most transplant centers delay therapy until recurrent hepatitis C in the transplanted liver is confirmed. Oral, highly effective, direct-acting antivirals have shown encouraging results in patients who have undergone liver transplantation for hepatitis C infection and have recurrent hepatitis C. The choice of therapy needs to be individualized and is rapidly evolving.
Once patients successfully complete treatment, the viral load after treatment determines if there is an SVR or cure. If cure is achieved (undetectable viral load after treatment), no further additional testing is recommended unless the patient has cirrhosis. Those who are not cured will need continued monitoring for progression of liver disease and its complications.
While cure eliminates worsening of fibrosis by hepatitis C, complications may still affect those with cirrhosis. These individuals still need regular screening for liver cancer as well as monitoring for esophageal varices that may bleed.
Because hepatitis B co-infection may reactivate or worsen even after treatment for HCV, monitoring for hepatitis symptoms may be needed after the end of therapy.
At this time there are no effective home or over-the-counter treatments for hepatitis C.
Over several years or decades, chronic inflammation may cause death of liver cells and cirrhosis (scaring, fibrosis). When the liver becomes cirrhotic, it becomes stiff, and it cannot perform its normal functions of clearing waste products from the blood. As fibrosis worsens, symptoms of liver failure begin to appear. This is called "decompensated cirrhosis " or "end-stage liver disease. " Symptoms of end-stage liver disease include:
The liver and spleen have an important function of clearing bacteria from the blood stream. Cirrhosis affects many areas of immune function, including attraction of white blood cells to bacteria, reduced killing of bacteria, reduced production of proteins involved in immune defenses, and decreased life span of white blood cells involved in immune defenses. This may be referred to as having cirrhosis-associated immune dysfunction syndrome or CAIDS.
Transmission of hepatitis C can be prevented in several ways.
Prevention programs aim at needle sharing among drug addicts. Needle exchange programs and education have reduced transmission of hepatitis C infection. However, IV drug users are a difficult to reach population, and rates of hepatitis C remain high among them.
Among health care workers, safe needle-usage techniques have been developed to reduce accidental needlesticks. Newer needle systems prevent manual recapping of needles after use of syringes, which is a frequent cause of accidental needlesticks
There is no clear way to prevent hepatitis C transmission from mother to fetus at this time.
People with multiple sexual partners should use barrier precautions such as condoms to limit the risk of hepatitis C and other sexually transmitted diseases, including HIV.
If one partner is infected, monogamous couples may want to consider the low risk of transmission of hepatitis C infection when deciding whether to use condoms during sex. Some couples may decide to use them and some may not.
Screening of the blood supply has almost eliminated the risk of transmission of hepatitis C infection through transfusion.
People with hepatitis C infection should not share razors or toothbrushes with others because of the possibility that these items may be contaminated with blood.
People who want to get a body piercing(s) or tattoo(s) are encouraged to do so only at licensed piercing and tattoo shops (facilities), and verify that the body piercing or tattoo shop uses infection-control practices.
It is critical that physicians and clinics follow manufacturers and regulatory agency directions for sterilizing/cleaning instruments and that disposable instruments be discarded properly. There is no need to use special isolation procedures when dealing with hepatitis C infected patients.
In general, among patients with untreated hepatitis C:
Drinking alcohol and acquiring other hepatitis viruses are risk factors for worse liver disease. People with chronic hepatitis C should avoid drinking alcohol and should be screened for antibodies to hepatitis A and B. If they do not have antibodies, they should be vaccinated against these other hepatitis viruses.
People with hepatitis C should be educated about preventing HIV infection. Infection with both HIV and hepatitis C speeds up and worsens liver damage caused by hepatitis C. Hepatitis C also can affect the HIV infection and how it is treated. About 25% of people with HIV infection are co-infected (also infected) with hepatitis C, and up to 90% of IV drug users with HIV are co-infected with hepatitis C. Screening for hepatitis viruses is important in all people infected with HIV, just as screening for HIV is important in people who have hepatitis C.
Liver cancer (hepatocellular carcinoma, or hepatoma) is associated with cirrhosis from chronic hepatitis C. Some experts recommend screening patients with hepatitis C infection and cirrhosis for liver cancer periodically.
As our knowledge of hepatitis C increases, more and more patients are being diagnosed with chronic infection. Current research is very active and includes diagnosis, natural history, treatment, and vaccine development. Thus the field is constantly changing, with new guidelines added frequently.
 Gastroenterólogo en Fort Pierce, Florida
Gastroenterólogo en Fort Pierce, Florida
 ¿Qué alimentos desencadenan la colitis ulcerosa?
¿Qué alimentos desencadenan la colitis ulcerosa?
 Síndrome de intestino permeable:¿la enfermedad que su médico no puede diagnosticar?
Síndrome de intestino permeable:¿la enfermedad que su médico no puede diagnosticar?
 Las propiedades únicas y los beneficios para la salud de los alimentos fermentados
Las propiedades únicas y los beneficios para la salud de los alimentos fermentados
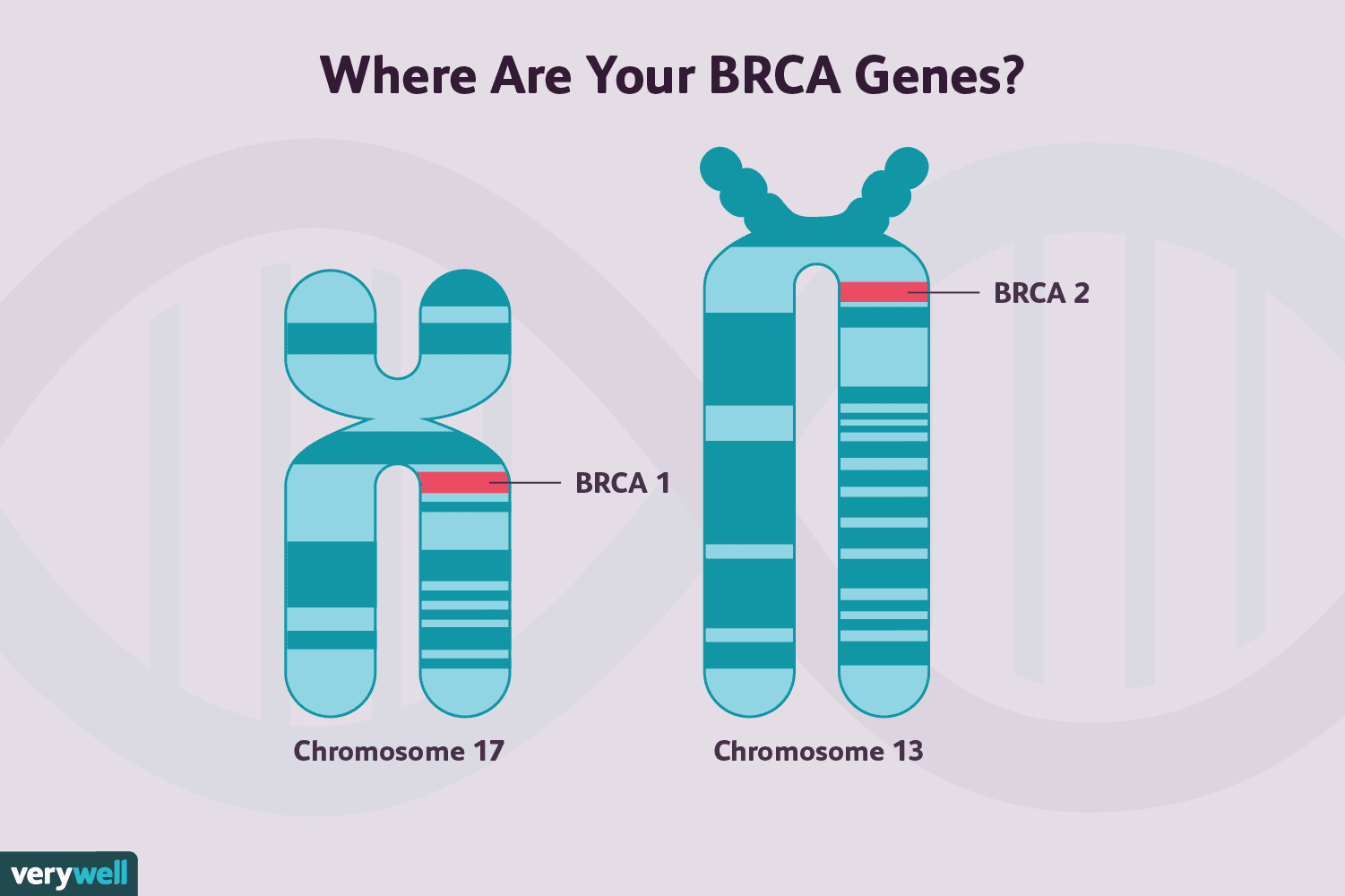 Mutaciones del gen no BRCA que aumentan el riesgo de cáncer de mama
Mutaciones del gen no BRCA que aumentan el riesgo de cáncer de mama
 Razones por las que puede necesitar una colonoscopia
Razones por las que puede necesitar una colonoscopia
 El ultrasonido es el mejor detector de embarazos ectópicos peligrosos, según un estudio
Últimas noticias sobre el embarazo Omitir la vacuna COVID en el embarazo Estas mujeres embarazadas enfrentan un alto riesgo de enfermedad cardíaca La lactancia materna protege el corazón de una madre
El ultrasonido es el mejor detector de embarazos ectópicos peligrosos, según un estudio
Últimas noticias sobre el embarazo Omitir la vacuna COVID en el embarazo Estas mujeres embarazadas enfrentan un alto riesgo de enfermedad cardíaca La lactancia materna protege el corazón de una madre
 Registros de interés del Programa de Coaching SIBO
Inscripciones de interés para el programa de entrenamiento SIBO ahora abiertas Mencioné la semana pasada que tenía algunas noticias emocionantes para compartir con ustedes. Estoy encantado de anuncia
Registros de interés del Programa de Coaching SIBO
Inscripciones de interés para el programa de entrenamiento SIBO ahora abiertas Mencioné la semana pasada que tenía algunas noticias emocionantes para compartir con ustedes. Estoy encantado de anuncia
 Mi antiguo yo debe morir (una carta abierta sobre mi divorcio)
Escribo esto como un adiós agradecido. Mi viejo yo debe morir. No estoy seguro de cómo decir esto, pero mereces saberlo:durante el último año, he estado pasando por un divorcio. La amo. Estoy agra
Mi antiguo yo debe morir (una carta abierta sobre mi divorcio)
Escribo esto como un adiós agradecido. Mi viejo yo debe morir. No estoy seguro de cómo decir esto, pero mereces saberlo:durante el último año, he estado pasando por un divorcio. La amo. Estoy agra