 Kas yra HCV, kaip juo užsikrečiama, ar yra simptomų ir ar ji išgydoma?
Kas yra HCV, kaip juo užsikrečiama, ar yra simptomų ir ar ji išgydoma?Dauguma žmonių, užsikrėtusių hepatitu C (hep C), neturi jokių simptomų. Tačiau tie, kurie turi simptomų, gali patirti:
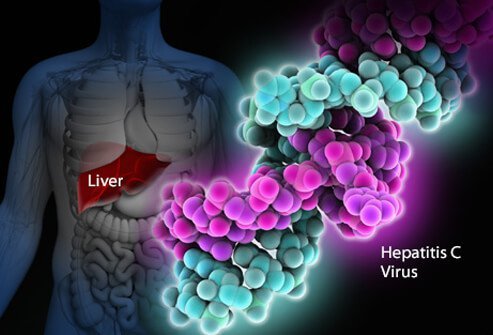
Hepatito C viruso infekcija yra kepenų infekcija, kurią sukelia hepatito C virusas (taip pat vadinamas HCV arba hep C). Žmogaus imuninei sistemai sunku pašalinti hepatitą C iš organizmo, o užsikrėtimas hepatitu C dažniausiai tampa lėtinis. Per dešimtmečius lėtinė hepatito C infekcija pažeidžia kepenis ir gali sukelti kepenų nepakankamumą. JAV CDC apskaičiavo, kad 2016 m. įvyko maždaug 41 200 naujų hepatito C atvejų. Kai virusas pirmą kartą patenka į organizmą, paprastai nėra jokių simptomų, todėl šis skaičius yra apytikslis. Apie 75–85% naujai užsikrėtusių žmonių užsikrečia chroniškai. Apskaičiuota, kad JAV daugiau nei 2 milijonai žmonių yra chroniškai užsikrėtę hepatitu C. Infekcija dažniausiai aptinkama tarp 40–60 metų amžiaus žmonių, o tai atspindi didelį užsikrėtimo lygį aštuntajame ir devintajame dešimtmečiuose. Kiekvienais metais JAV miršta nuo 8 000 iki 10 000 nuo hepatito C infekcijos. HCV infekcija yra pagrindinė kepenų transplantacijos priežastis JAV ir yra kepenų vėžio rizikos veiksnys. 2016 m. 18 153 mirties liudijimuose HCV buvo nurodyta kaip pagrindinė mirties priežastis; Manoma, kad tai nepakankamai įvertinta.
Maždaug 10–20 % sergančiųjų lėtiniu HCV susirgs ciroze per 20–30 metų. Kepenų cirozės progresavimą gali paspartinti vyresni nei 50 metų amžiaus, vyriškos lyties, alkoholio vartojimo, nealkoholinės suriebėjusių kepenų ligos (NASH), gretutinės hepatito B ar ŽIV infekcijos ir imunitetą slopinančių vaistų buvimas. HCV infekcija yra pagrindinė kepenų persodinimo priežastis dėl kepenų nepakankamumo JAV
Tie, kurie serga ciroze dėl HCV, taip pat turi kasmet apie 1–5% kepenų vėžio (hepatomos arba hepatoceliulinės karcinomos) riziką.
Hepatitas reiškia kepenų uždegimą. Hepatitas C yra vienas iš kelių virusų, galinčių sukelti virusinį hepatitą. Jis nesusijęs su kitais įprastais hepatito virusais (pavyzdžiui, hepatitu A arba hepatitu B). Hepatitas C yra Flaviviridae narys virusų šeima. Kiti šios virusų šeimos nariai yra tie, kurie sukelia geltonąją karštligę ir dengės karštligę.
Yra mažiausiai šeši skirtingi viruso genotipai (štamos), kurie turi skirtingus genetinius profilius (nuo 1 iki 6 genotipų). JAV 1 genotipas yra labiausiai paplitusi hepatito C padermė. Net ir viename genotipe gali būti tam tikrų variacijų (pavyzdžiui, 1a ir 1b genotipai). Genotipų nustatymas naudojamas gydymui, nes kai kurie viruso genotipai geriau reaguoja į kai kuriuos gydymo būdus nei į kitus.
Kaip ir žmogaus imunodeficito virusas (ŽIV), hepatitas C dauginasi labai greitai ir pasiekia labai aukštą lygį organizme. Genai, dėl kurių susidaro viruso paviršiaus baltymai, taip pat greitai mutuoja (kinta), o kasdien susidaro tūkstančiai viruso genetinių variantų („kvazirūšių“). Kūnas negali neatsilikti nuo anti-HCV antikūnų prieš visas vienu metu cirkuliuojančias kvazi rūšis. Dar nebuvo įmanoma sukurti veiksmingos vakcinos, nes vakcina turi apsaugoti nuo visų genotipų.
Hepatito C infekcija kepenyse suaktyvina imuninę sistemą, o tai sukelia uždegimą. Maždaug 20–30% ūmiai užsikrėtusių asmenų patirs tipiškus hepatito simptomus, tokius kaip pilvo skausmas, gelta, tamsus šlapimas arba molio spalvos išmatos. Tačiau lėtinis hepatitas C paprastai nesukelia jokių simptomų iki ligos pabaigos, o hepatitu C sergantys žmonės vadina „miegančiu drakonu“. Per kelerius metus ar dešimtmečius lėtinis uždegimas gali sukelti kepenų ląstelių mirtį ir randus ("fibrozę"). Dideli randai kepenyse vadinami ciroze. Dėl to laipsniškai pažeidžiamos gyvybinės kepenų funkcijos. Kepenys, sergančios ciroze, yra labiau linkusios į kepenų vėžį. Alkoholio vartojimas pagreitina kepenų pažeidimą sergant hepatitu C. Kartu užsikrėtusi ŽIV infekcija, taip pat ūminė hepatito A ar B infekcija, taip pat paspartins cirozės progresavimą.
Maždaug 70–80% žmonių pirmą kartą užsikrėtę HCV nejaučia jokių simptomų. Likę 20–30 % gali turėti
Ankstyvieji hepatito C simptomai gali būti tamsus šlapimas, geltonos akys arba molio spalvos išmatos, nors tai neįprasta. Laikui bėgant žmonėms, sergantiems lėtine HCV infekcija, gali atsirasti kepenų uždegimo požymių, rodančių, kad infekcija gali būti. Užsikrėtę asmenys gali lengvai pavargti arba skųstis nespecifiniais simptomais. Vėlesnių cirozės simptomų ir požymių dažnai nėra, kol uždegimas nėra pakankamai pažengęs. Kai cirozė progresuoja, simptomai ir požymiai didėja ir gali būti:
Kadangi hepatitu C užsikrečiama per kraują, specifinio užkrečiamumo laikotarpio nėra. Žmonės, kuriems išsivysto lėtinis hepatitas C, nešioja virusą kraujyje, todėl yra užkrečiami kitiems visą gyvenimą, nebent jie būtų išgydyti nuo hepatito C.
Sunku tiksliai pasakyti, koks yra hepatito C inkubacinis laikotarpis, nes daugumai hepatitu C užsikrėtusių žmonių ankstyvoje infekcijos stadijoje simptomai nepasireiškia. Tie, kuriems simptomai pasireiškia anksti po užsikrėtimo (vidutiniškai nuo 2 iki 12 savaičių, bet gali trukti ilgiau), pasireiškia lengvi virškinimo trakto simptomai, dėl kurių nereikia kreiptis į gydytoją.
Dauguma hepatito C infekcijos požymių ir simptomų yra susiję su kepenimis. Rečiau hepatito C infekcija gali paveikti kitus organus, išskyrus kepenis.
Hepatito C infekcija gali sukelti nenormalių antikūnų, vadinamų krioglobulinais, gamybą. Krioglobulinai sukelia arterijų uždegimą (vaskulitą). Tai gali pažeisti odą, sąnarius ir inkstus. Pacientams, sergantiems krioglobulinemija (krioglobulinų kiekis kraujyje), gali būti
Be to, užsikrėtusiems asmenims, sergantiems krioglobulinemija, gali išsivystyti Raynaud reiškinys, kai rankų ir kojų pirštai pasidaro spalvoti (balti, tada violetiniai, tada raudoni) ir tampa skausmingi esant žemai temperatūrai.
JAV prevencinių sveikatos tarnybų darbo grupė rekomenduoja visiems suaugusiems, gimusiems 1945–1965 m., kartą reguliariai tikrintis dėl hepatito C, neatsižvelgiant į tai, ar yra hepatito C rizikos veiksnių. Vienkartinis testavimas taip pat rekomenduojamas:
Žmonėms, kurie galėjo būti užsikrėtę hepatitu C per pastaruosius 6 mėnesius, reikia tirti viruso RNR kiekį, o ne anti-HCV antikūnus, nes antikūnų gali nebūti iki 12 savaičių ar ilgiau po užsikrėtimo, nors HCV RNR gali būti aptinkama. kraujyje praėjus 2-3 savaitėms po užsikrėtimo.
Apskritai kasmetinė patikra gali būti tinkama žmonėms, turintiems nuolatinių rizikos veiksnių, pvz., pasikartojančių lytiniu keliu plintančių ligų (LPL) arba daug lytinių partnerių, nuolat vartojantiems IV narkotikus arba ilgalaikiams hepatitu C sergančių žmonių sekso partneriams. Ar atlikti tyrimą, ar ne. šie žmonės nustatomi kiekvienu konkrečiu atveju.
Kiekvieno nėštumo metu HCV perdavimo iš motinos kūdikiui rizika yra 4–7%. Šiuo metu CDC nėra rekomendacijų dėl įprastinio hepatito C patikrinimo nėštumo metu ir šiuo metu nėra rekomenduojamo vaisto, kuris apsaugotų nuo perdavimo iš motinos kūdikiui (profilaktika). Tačiau CDC stebi tyrimų rezultatus ir gali pateikti rekomendacijų ateityje, kai atsiras įrodymų.
Nors duomenys vis dar riboti, neseniai Jungtinėje Karalystėje atliktas daugiau nei 1000 atvejų tyrimas parodė, kad 11 % kūdikių buvo užsikrėtę gimimo metu ir šiems kūdikiams cirozė gali išsivystyti būdami 30 metų amžiaus. HCV atrankos nėštumo metu atvejis apima galimybę saugiai gydyti motinas nėštumo metu tiesioginio veikimo antivirusiniais vaistais (DAA), kad būtų galima gydyti motiną prieš cirozei išsivystant, užkirsti kelią kūdikių perdavimui ir užkirsti kelią perdavimui kitiems. Vaikai, gimę HCV infekuotų motinų, taip pat gali būti gydomi ankstyvame amžiuje, kad būtų išvengta cirozės ir perdavimo kitiems. Norint pasiekti šiuos tikslus, bus svarbus kelių specialistų priežiūros koordinavimas.
HCV infekuotų motinų vaikai gali būti tikrinami dėl hepatito C jau nuo 1-2 mėnesių amžiaus, naudojant hepatito C viruso kiekį arba PGR tyrimus (žr. Hepatito C kraujo tyrimai). Antikūnai prieš hepatitą C, perduodami iš motinos vaikui, išliks iki 18 mėnesių, todėl vaikai turi būti tiriami dėl HCV antikūnų ne anksčiau.
Hepatitą C gydo arba gastroenterologas, ir hepatologas (gastroenterologas, turintis papildomą išsilavinimą kepenų ligų srityje) arba infekcinių ligų specialistas. Gydymo komandą gali sudaryti daugiau nei vienas specialistas, atsižvelgiant į kepenų pažeidimo mastą. Chirurgai, kurie specializuojasi kepenų chirurgijoje, įskaitant kepenų transplantaciją, yra medicinos komandos dalis ir turėtų priimti pacientus, sergančius pažengusia liga (kepenų nepakankamumu ar ciroze). anksti, kol pacientui prireikė kepenų persodinimo. Jie gali nustatyti problemas, kurias reikia išspręsti prieš pradedant svarstyti operaciją. Kiti asmenys, galintys padėti gydyti pacientus, yra dietologai, kurie konsultuoja mitybos klausimais, ir vaistininkai, padedantys valdyti vaistus.
Yra keli kraujo tyrimai, skirti diagnozuoti hepatito C infekciją. Kraujas gali būti tiriamas dėl antikūnų prieš hepatitą C (anti-HCV antikūnas). Vidutiniškai užtrunka apie 8–12 savaičių ir iki 6 mėnesių, kol po pirminės užsikrėtimo hepatitu C susiformuoja antikūnai, todėl atliekant antikūnų patikrą gali trūkti kelių naujai užsikrėtusių asmenų. Antikūnų buvimas nėra absoliutus aktyvaus, besidauginančio hepatito C viruso požymis, tačiau jei antikūnų testas yra teigiamas (antikūnų yra), statistinė aktyvios infekcijos tikimybė yra didesnė nei 99%.
Yra keletas testų, leidžiančių nustatyti hepatito C viruso kiekį žmogaus kraujyje (viruso apkrovą). Hepatito C viruso RNR galima nustatyti atliekant tyrimą, vadinamą polimerazės grandinine reakcija (PGR), kuris aptinka kraujyje cirkuliuojantį virusą praėjus 2–3 savaitėms po užsikrėtimo, todėl jį galima naudoti nustatant įtariamą ūmią hepatito C infekciją. ankstyva infekcija. Jis taip pat naudojamas siekiant nustatyti, ar asmuo, turintis antikūnų prieš hepatitą C, serga aktyviu hepatitu, ir stebėti viruso kiekį gydymo metu.
Taip pat atliekami kraujo tyrimai, siekiant nustatyti HCV genotipus. Genotipai skirtingai reaguoja į skirtingą gydymą, todėl ši informacija yra svarbi renkantis tinkamiausią gydymo režimą.
Kepenų fibrozės įvertinimas naudojant kraujo tyrimus taip pat yra gana patikimas diagnozuojant kliniškai reikšmingus randus; tai FIB-4, FibroSure, Fibrotest ir aspartato aminotransferazės ir trombocitų santykio indeksas (APRI).
Kitas žingsnis yra nustatyti kepenų randų lygį. Kepenų biopsija leidžia ištirti nedidelį kepenų audinio mėginį mikroskopu, tačiau kepenų biopsija yra invazinis tyrimas ir kelia didelę kraujavimo riziką. Ankstyvosios ligos metu taip pat gali nepastebėti nenormalių sričių.
Neinvaziniai tyrimai iš esmės pakeitė kepenų biopsiją, išskyrus ypatingas situacijas. Liver stiffness indicates that advanced liver scarring or cirrhosis may be present. Transient elastography may be used to measure this stiffness by ultrasound or magnetic resonance imaging (MRI).
Pre-treatment evaluation for hepatitis C also should include:
Interferons, for example, Roferon-A and Infergen, and pegylated interferons such as Peg-Intron T , Pegasys, were mainstays of treatment for years. Interferons produced sustained viral response (SVR, or cure) of up to 15%. Later, peglatedll forms produced SVR of 50%-80%. These drugs were injected, had many adverse effects, required frequent monitoring, and were often combined with oral ribavirin, which caused anemia. Treatment durations ranged up to 48 weeks.
Direct-acting anti-viral agents (DAAs) are antiviral drugs that act directly on hepatitis C multiplication.
Hepatitis C treatment is best discussed with a doctor or specialist familiar with current and developing options as this field is changing, and even major guidelines may become outdated quickly.
The latest treatment guidelines by the American Association for the Study of Liver Disease (AASLD) and Infectious Disease Society of America (IDSA) recommends use of DAAs as first-line treatment for hepatitis C infection. The choice of DAA varies by specific virus genotype, and the presence or absence of cirrhosis. In the U.S., specific insurance providers also might influence the choice due to the high cost of DAAs. Although the individual, public health, and cost benefits of treating all patients with hepatitis C is clear, the most difficult barrier to treating all people with HCV is the very high cost of the drug regimens. Patients are encouraged to discuss options with their health care professional.
Treatment is recommended in all patients with chronic hepatitis C unless they have a short life expectancy that is not related to liver disease. Severe life-threatening liver disease may require liver transplantation. Newer therapies with DAAs have allowed more and more patients to be treated.
The ultimate goals of antiviral therapy are to
A side goal is preventing co-infections with other hepatitis viruses, such as A and B, which can cause more liver disease than HCV alone. These can be prevented by vaccines and treatment.
When people first get hepatitis C, the infection is said to be acute. Most people with acute hepatitis C do not have symptoms so they are not recognized as being infected. However, some have low-grade fever, fatigue or other symptoms that lead to an early diagnosis. Others who become infected and have a known exposure to an infected source, such as a needlestick injury, are monitored closely.
Treatment decisions should be made on a case-by-case basis. Response to treatment is higher in acute hepatitis infection than chronic infection. However, many experts prefer to hold off treatment for 8-12 weeks to see whether the patient naturally eliminates the virus without treatment. Approaches to treatment are evolving. Patients with acute hepatitis C infection should discuss treatment options with a health care professional who is experienced in treating the disease. There is no established treatment regimen at this time.
If the hepatitis C RNA remains undetectable at the end of the treatment and follow-up period, this is called a sustained virologic response (SVR) and is considered a cure. Over 90% of people treated with DAAs are cured. These people have significantly reduced liver inflammation, and liver scarring may even be reversed.
About 5% of people who are treated for HCV infection are not cured by some of the older regimens. These people may still have options for cure with the newer regimens.
Few people with hepatitis C are at risk for problems if they are treated, however there are some factors that affect treatment regimens, such as concurrent HIV medications and kidney dysfunction. Some drugs are not safe for people with cirrhosis. Individuals who are unable to comply with the treatment schedule for psychological reasons or ongoing drug or alcohol abuse may not be good candidates for treatment because the drugs are very costly and require adherence to the pill regimen and regular follow-up visits. There are some important drug interactions with some of the medications that should be considered by the health care professional.
People with past hepatitis B or who have chronic active hepatitis B should not be treated for HCV without treating for HBV as well. As highly effective treatment for HCV has emerged, reports of serious hepatitis B have come to light. Similar to HCV, hepatitis B usually does not clear from the liver after acute infection, even though it is far less likely to cause chronic active hepatitis than hepatitis C infection. It remains dormant in most people, but it can reactivate with changes in the immune system. It is not clear why eliminating the HCV can allow the HBV infection to flare up. Hepatitis B screening is an important part of the hepatitis C evaluation. Those who have laboratory evidence of active or past infection with HBV should be monitored while receiving HCV treatment.
Compared to interferons and ribavirin drugs, the side effects of DAAs are far fewer and more tolerable. These side effects usually do not require discontinuation of therapy and are self-limiting after completion of therapy.
Patients with hepatitis B co-infection should be monitored for symptoms of reactivation of hepatitis, which are the same as the symptoms of acute hepatitis. The treating doctor may perform blood screening for this as well.
Hepatitis C is the leading reason for 40% to 45% of liver transplants in the U.S. Hepatitis C usually recurs after transplantation and infects the new liver. Approximately 25% of these patients with recurrent hepatitis will develop cirrhosis within five years of transplantation. Despite this, the five-year survival rate for patients with hepatitis C is similar to that of patients who are transplanted for other types of liver disease.
Most transplant centers delay therapy until recurrent hepatitis C in the transplanted liver is confirmed. Oral, highly effective, direct-acting antivirals have shown encouraging results in patients who have undergone liver transplantation for hepatitis C infection and have recurrent hepatitis C. The choice of therapy needs to be individualized and is rapidly evolving.
Once patients successfully complete treatment, the viral load after treatment determines if there is an SVR or cure. If cure is achieved (undetectable viral load after treatment), no further additional testing is recommended unless the patient has cirrhosis. Those who are not cured will need continued monitoring for progression of liver disease and its complications.
While cure eliminates worsening of fibrosis by hepatitis C, complications may still affect those with cirrhosis. These individuals still need regular screening for liver cancer as well as monitoring for esophageal varices that may bleed.
Because hepatitis B co-infection may reactivate or worsen even after treatment for HCV, monitoring for hepatitis symptoms may be needed after the end of therapy.
At this time there are no effective home or over-the-counter treatments for hepatitis C.
Over several years or decades, chronic inflammation may cause death of liver cells and cirrhosis (scaring, fibrosis). When the liver becomes cirrhotic, it becomes stiff, and it cannot perform its normal functions of clearing waste products from the blood. As fibrosis worsens, symptoms of liver failure begin to appear. This is called "decompensated cirrhosis " or "end-stage liver disease. " Symptoms of end-stage liver disease include:
The liver and spleen have an important function of clearing bacteria from the blood stream. Cirrhosis affects many areas of immune function, including attraction of white blood cells to bacteria, reduced killing of bacteria, reduced production of proteins involved in immune defenses, and decreased life span of white blood cells involved in immune defenses. This may be referred to as having cirrhosis-associated immune dysfunction syndrome or CAIDS.
Transmission of hepatitis C can be prevented in several ways.
Prevention programs aim at needle sharing among drug addicts. Needle exchange programs and education have reduced transmission of hepatitis C infection. However, IV drug users are a difficult to reach population, and rates of hepatitis C remain high among them.
Among health care workers, safe needle-usage techniques have been developed to reduce accidental needlesticks. Newer needle systems prevent manual recapping of needles after use of syringes, which is a frequent cause of accidental needlesticks
There is no clear way to prevent hepatitis C transmission from mother to fetus at this time.
People with multiple sexual partners should use barrier precautions such as condoms to limit the risk of hepatitis C and other sexually transmitted diseases, including HIV.
If one partner is infected, monogamous couples may want to consider the low risk of transmission of hepatitis C infection when deciding whether to use condoms during sex. Some couples may decide to use them and some may not.
Screening of the blood supply has almost eliminated the risk of transmission of hepatitis C infection through transfusion.
People with hepatitis C infection should not share razors or toothbrushes with others because of the possibility that these items may be contaminated with blood.
People who want to get a body piercing(s) or tattoo(s) are encouraged to do so only at licensed piercing and tattoo shops (facilities), and verify that the body piercing or tattoo shop uses infection-control practices.
It is critical that physicians and clinics follow manufacturers and regulatory agency directions for sterilizing/cleaning instruments and that disposable instruments be discarded properly. There is no need to use special isolation procedures when dealing with hepatitis C infected patients.
In general, among patients with untreated hepatitis C:
Drinking alcohol and acquiring other hepatitis viruses are risk factors for worse liver disease. People with chronic hepatitis C should avoid drinking alcohol and should be screened for antibodies to hepatitis A and B. If they do not have antibodies, they should be vaccinated against these other hepatitis viruses.
People with hepatitis C should be educated about preventing HIV infection. Infection with both HIV and hepatitis C speeds up and worsens liver damage caused by hepatitis C. Hepatitis C also can affect the HIV infection and how it is treated. About 25% of people with HIV infection are co-infected (also infected) with hepatitis C, and up to 90% of IV drug users with HIV are co-infected with hepatitis C. Screening for hepatitis viruses is important in all people infected with HIV, just as screening for HIV is important in people who have hepatitis C.
Liver cancer (hepatocellular carcinoma, or hepatoma) is associated with cirrhosis from chronic hepatitis C. Some experts recommend screening patients with hepatitis C infection and cirrhosis for liver cancer periodically.
As our knowledge of hepatitis C increases, more and more patients are being diagnosed with chronic infection. Current research is very active and includes diagnosis, natural history, treatment, and vaccine development. Thus the field is constantly changing, with new guidelines added frequently.
 pagaminkite šį vakarą:vaikinams tinkami čili con carne
Šią savaitę pripildykite savo namus šiltu prieskonių aromatu. Šiandienos SIBO kulinarijos laidos serija su Rebecca Coomes yra tikras jaudulys, kai ji perkelia jus į savo minią džiuginantį chili con ca
pagaminkite šį vakarą:vaikinams tinkami čili con carne
Šią savaitę pripildykite savo namus šiltu prieskonių aromatu. Šiandienos SIBO kulinarijos laidos serija su Rebecca Coomes yra tikras jaudulys, kai ji perkelia jus į savo minią džiuginantį chili con ca
 Kokie maisto produktai sukelia opinį kolitą?
Kaip man pradėti rasti tinkamą dietą opiniam kolitui gydyti? Opinis kolitas (arba uždegiminė žarnyno liga) yra būklė, su kuria sunku gyventi. Maisto produktai, sukeliantys opinį kolitą, yra žalios
Kokie maisto produktai sukelia opinį kolitą?
Kaip man pradėti rasti tinkamą dietą opiniam kolitui gydyti? Opinis kolitas (arba uždegiminė žarnyno liga) yra būklė, su kuria sunku gyventi. Maisto produktai, sukeliantys opinį kolitą, yra žalios
 Ar tai dirgliosios žarnos sindromas?
Ar žinojote, kad balandis yra dirgliosios žarnos sindromo (IBS) supratimo mėnuo? „Ignite“ daugiausia užsiimu funkciniais žarnyno sutrikimais ir kitomis žarnyno ligomis. DŽS man yra labai artimas ir b
Ar tai dirgliosios žarnos sindromas?
Ar žinojote, kad balandis yra dirgliosios žarnos sindromo (IBS) supratimo mėnuo? „Ignite“ daugiausia užsiimu funkciniais žarnyno sutrikimais ir kitomis žarnyno ligomis. DŽS man yra labai artimas ir b