 Wat ass HCV, wéi gëtt et iwwerdroen, ginn et Symptomer, an ass et geheelt?
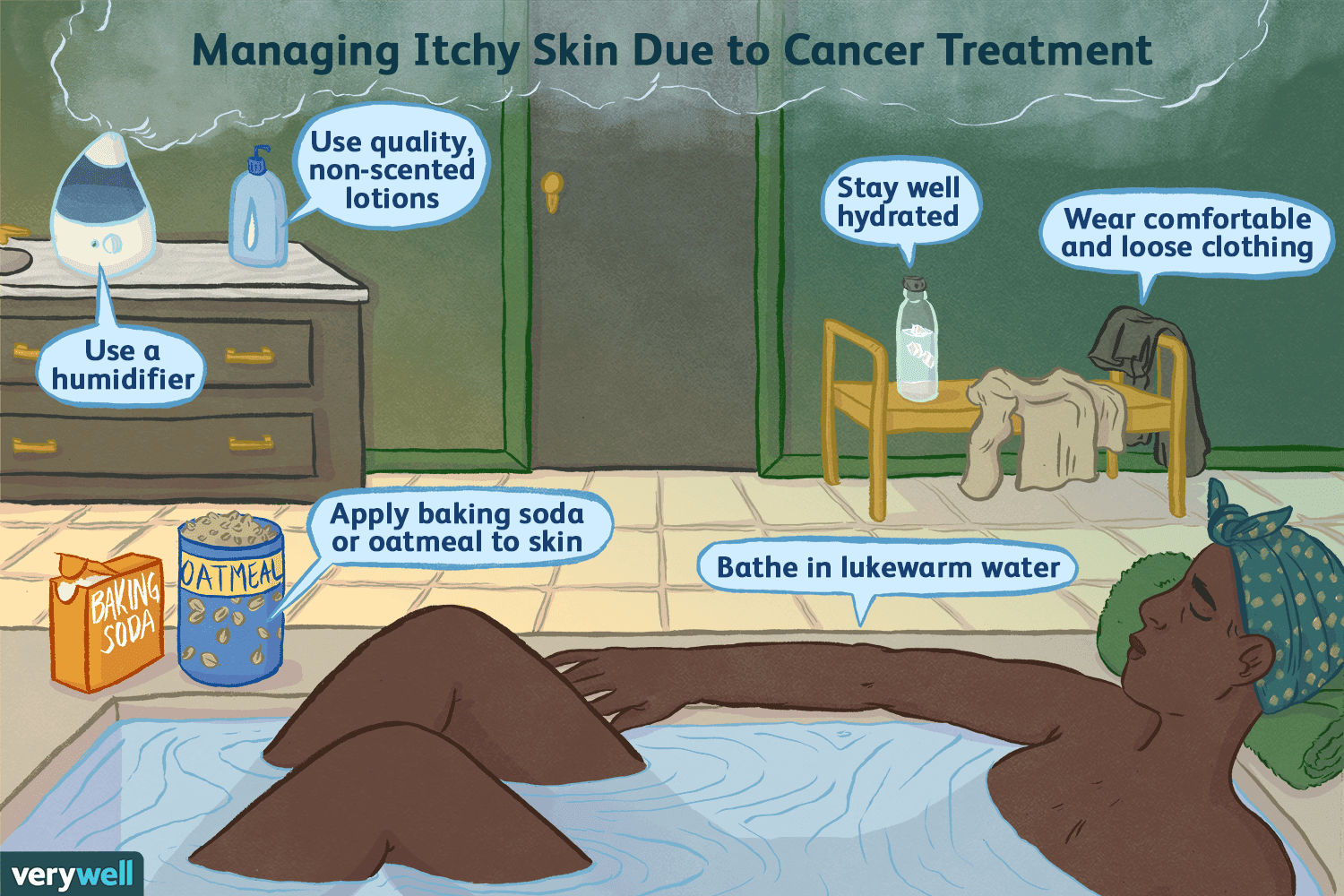
Wat ass HCV, wéi gëtt et iwwerdroen, ginn et Symptomer, an ass et geheelt?Déi meescht Leit, déi Hepatitis C (hep C) optrieden, hu keng Symptomer. Wéi och ëmmer, déi, déi Symptomer hunn, kënnen erliewen:
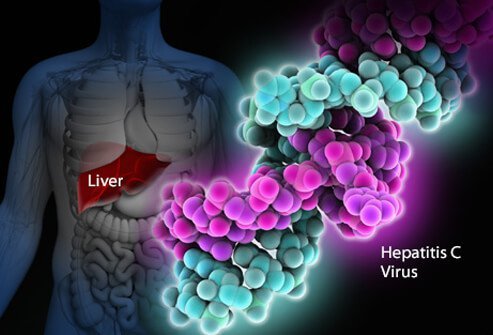
Hepatitis C Virus Infektioun ass eng Infektioun vun der Liewer verursaacht duerch den Hepatitis C Virus (och als HCV oder Hep C bezeechent). Et ass schwéier fir de mënschlechen Immunsystem Hepatitis C aus dem Kierper ze eliminéieren, an Infektioun mat Hepatitis C gëtt normalerweis chronesch. Iwwer Joerzéngte, chronesch Infektioun mat Hepatitis C beschiedegt d'Liewer a kann Leberfehler verursaachen. An den USA huet d'CDC geschat datt ongeféier 41.200 nei Fäll vun Hepatitis C am Joer 2016 geschitt sinn. Wann de Virus fir d'éischt an de Kierper erakënnt, ginn et normalerweis keng Symptomer, sou datt dës Zuel eng Schätzung ass. Ongeféier 75% -85% vun nei infizéierte Leit ginn chronesch infizéiert. An den USA gi geschat datt méi wéi 2 Millioune Leit chronesch mat Hepatitis C infizéiert sinn. D'Infektioun gëtt am meeschte verbreet ënner Leit déi 40 bis 60 Joer al sinn, wat déi héich Infektiounsraten an den 1970er an 1980er reflektéiert. Et ginn 8.000 bis 10.000 Doudesfäll all Joer an den USA am Zesummenhang mat der Hepatitis C Infektioun. HCV Infektioun ass déi Haaptursaach vun der Lebertransplantatioun an den USA an ass e Risikofaktor fir Lebererkrank. Am Joer 2016 hunn 18.153 Doudeszertifikater HCV als bäitragend Doudesursaach opgelëscht; dat gëtt ugeholl datt et eng Ënnerschätzung ass.
Ongeféier 10% -20% vun deenen, déi chronesch HCV entwéckelen, entwéckelen Zirrhose bannent 20-30 Joer. De Fortschrëtt zu Zirrhose kann duerch Alter iwwer 50 beschleunegt ginn, männlecht Geschlecht, Alkoholkonsum, net-alkoholesch Fettleberkrankheet (NASH), Co-Infektioun mat Hepatitis B oder HIV, an Immun-ënnerdréckende Medikamenter. HCV Infektioun ass déi Haaptursaach vun der Lebertransplantatioun wéinst Leberfehler an den USA.
Déi, déi Zirrhose vum HCV hunn, hunn och e jäerleche Risiko vu Liewerkriibs (Hepatom oder Hepatozellulär Karzinom) vun ongeféier 1% -5%.
Hepatitis heescht Entzündung vun der Liewer. Hepatitis C ass ee vu ville Viren déi viral Hepatitis verursaache kënnen. Et ass net verwandt mat den anere gemeinsame Hepatitis Viren (zum Beispill Hepatitis A oder Hepatitis B). Hepatitis C ass Member vun der Flaviviridae Famill vu Viren. Aner Membere vun dëser Famill vu Viren enthalen déi, déi giel Féiwer an Dengue Féiwer verursaachen.
Et ginn op d'mannst sechs verschidde Genotypen (Stämme) vum Virus déi verschidde genetesch Profiler hunn (Genotypen 1 bis 6). An den USA ass Genotyp 1 déi heefegst Stamm vun Hepatitis C. Och an engem eenzegen Genotyp kënnen et e puer Variatiounen sinn (Genotyp 1a an 1b, zum Beispill). Genotyping gëtt benotzt fir d'Behandlung ze guidéieren, well verschidde virale Genotypen besser op e puer Therapien reagéieren wéi op anerer.
Wéi de Mënsch Immunodeficiency Virus (HIV), Hepatitis C multiplizéiert ganz séier an erreecht ganz héich Niveauen am Kierper. D'Gen, déi d'Uewerflächeproteine vum Virus maachen, mutéieren (veränneren) och séier, an Dausende vun genetesch Variatiounen vum Virus ("quasi-Arten") ginn all Dag produzéiert. Et ass onméiglech fir de Kierper ze halen mat der Produktioun vun Anti-HCV Antikörper géint all quasi Arten déi gläichzäiteg zirkuléieren. Et war nach net méiglech eng effektiv Impfung z'entwéckelen, well d'Impfung muss géint all Genotypen schützen.
Hepatitis C Infektioun an der Liewer dréit den Immunsystem aus, wat zu Entzündung féiert. Ongeféier 20% -30% vun deenen akut infizéiert erliewen typesch Hepatitis Symptomer wéi Bauchschmerzen, Geel, donkel Urin oder Lehmfaarweg Hocker. Wéi och ëmmer, chronesch Hepatitis C verursaacht normalerweis keng Symptomer bis ganz spéit an der Krankheet, an Hepatitis C gouf vu Patienten als de "schlofen Draach" bezeechent. Iwwer e puer Joer oder Joerzéngte kann chronesch Entzündung Doud vu Liewerzellen a Narben verursaachen ("Fibrose"). Extensiv Narben an der Liewer gëtt Zirrhose genannt. Dëst behënnert progressiv vital Funktiounen vun der Liewer. Zirrhotesch Liewer si méi ufälleg fir Liewerkriibs. Alkohol drénken beschleunegt d'Leberschued mat Hepatitis C. Gläichzäiteg HIV Infektioun, souwéi akuter Hepatitis A oder B Infektioun, wäerten och de Fortschrëtt zu Zirrhose beschleunegen.
Ongeféier 70% -80% vun de Leit hu keng Symptomer wann se fir d'éischt HCV Infektioun kréien. Déi reschtlech 20%-30% hu vläicht
Fréier Symptomer vun Hepatitis C kënnen donkel Urin, giel Aen oder Lehmfaarweg Hocker enthalen, obwuel dëst ongewéinlech ass. Mat der Zäit kënne Leit mat chronescher HCV Infektioun Zeeche vun der Leberentzündung entwéckelen, déi suggeréiert datt d'Infektioun präsent ass. Infizéiert Individuen kënne liicht midd ginn oder beschwéieren iwwer net spezifesch Symptomer. Déi spéider Symptomer an Zeeche vun der Zirrhose sinn dacks fehlt bis d'Entzündung zimlech fortgeschratt ass. Wéi d'Zirrhose weidergeet, ginn d'Symptomer an d'Schëlder erop a kënnen enthalen:
Well Hepatitis C duerch Belaaschtung u Blutt iwwerdroe gëtt, gëtt et keng spezifesch Period vun der Ustiechung. Leit, déi chronesch Hepatitis C entwéckelen, droen de Virus an hirem Blutt an dofir si fir anerer hir ganzt Liewen ustiechend, ausser se vun hirer Hepatitis C geheelt ginn.
Dëst ass schwéier fir sécher ze soen wat d'Inkubatiounszäit fir Hepatitis C ass, well déi meescht Leit, déi mat Hepatitis C infizéiert sinn, keng Symptomer fréi am Laf vun der Infektioun hunn. Déi, déi Symptomer fréi entwéckelen nodeems se infizéiert sinn (2 bis 12 Wochen am Duerchschnëtt, awer kënne méi laang sinn) erliewen mild gastrointestinal Symptomer, déi vläicht net en Dokter besichen.
Déi meescht vun de Schëlder a Symptomer vun der Hepatitis C Infektioun bezéien sech op d'Liewer. Manner dacks, Hepatitis C Infektioun kann aner Organer wéi d'Liewer beaflossen.
Hepatitis C Infektioun kann de Kierper verursaachen anormal Antikörper genannt Cryoglobuline ze produzéieren. Cryoglobuline verursaachen Entzündung vun Arterien (Vaskulitis). Dëst kann Haut, Gelenker an Nieren beschiedegen. Patienten mat Kryoglobulinemie (Cryoglobulinen am Blutt) kënnen
Zousätzlech kënnen infizéiert Individuen mat Kryoglobulinemie dem Raynaud säi Phänomen entwéckelen, an deem d'Fanger an d'Zänn Faarf ginn (wäiss, dann violett, dann rout), a bei kalen Temperaturen schmerzhaf ginn.
D'US Preventive Health Services Task Force recommandéiert datt all Erwuessener gebuer tëscht 1945 an 1965 eemol routinéiert fir Hepatitis C getest ginn, egal ob Risikofaktoren fir Hepatitis C präsent sinn. Eemol Tester ass och recommandéiert fir:
Leit, déi an de leschte 6 Méint un Hepatitis C ausgesat waren, solle fir viral RNA Belaaschtung getest ginn anstatt Anti-HCV Antikörper, well Antikörper vläicht bis zu 12 Wochen oder méi no der Infektioun net präsent sinn, obwuel HCV RNA detektéierbar ka sinn am Blutt esou séier wéi 2-3 Wochen no der Infektioun.
Am Allgemengen, kann alljährlechen Duerchmusterung gëeegent sinn fir Leit mat lafende Risiko Faktoren wéi widderholl sexuell iwwerdroen Krankheeten (STDs) oder vill Sex Partner, lafend IV Drogenofhängeger benotzen, oder laangfristeg Sex Partner vun Leit mat Hepatitis C. Ob Test oder net dës Leit ginn op eng Entscheedung vu Fall zu Fall bestëmmt.
Et besteet e 4% -7% Risiko fir HCV vun der Mamm op d'Kand mat all Schwangerschaft ze iwwerdroen. De Moment gëtt et keng CDC Empfehlung fir Routine Hepatitis C Screening während der Schwangerschaft, an et gëtt keng aktuell empfohlene Medizin fir d'Transmissioun vu Mamm op Puppelcher (Prophylaxie) ze vermeiden. Wéi och ëmmer, CDC iwwerwaacht Fuerschungsresultater a kann Empfehlungen an Zukunft maachen wéi Beweiser entstinn.
Wärend d'Donnéeën nach ëmmer limitéiert sinn, huet eng rezent Studie vun iwwer 1.000 Fäll a Groussbritannien festgestallt datt 11% vun de Puppelcher bei der Gebuert infizéiert waren, an datt dës Puppelcher méiglecherweis Zirrhose an de fréie 30er entwéckelen. De Fall fir Screening fir HCV während der Schwangerschaft beinhalt d'Potenzial fir Mammen während der Schwangerschaft sécher ze behandelen mat direkten wierksamen antiviralen Agenten (DAAs) fir d'Mamm ze behandelen ier d'Zirrhose entwéckelt, d'Kandiwwerdroung ze verhënneren an d'Transmissioun un anerer ze verhënneren. Kanner gebuer zu HCV-infizéierte Mammen kënnen och an engem fréien Alter Behandlung ugebuede ginn fir Zirrhose ze vermeiden, souwéi Iwwerdroung un anerer. Koordinatioun vun der Betreiung tëscht verschidde Spezialisten wäert wichteg sinn fir dës Ziler z'erreechen.
Kanner vun HCV-infizéierte Mammen kënnen op Hepatitis C sou fréi wéi 1-2 Méint al mat Hepatitis C virale Last oder PCR Tester ënnersicht ginn (kuckt Blutt Tester fir Hepatitis C). Antikörper géint Hepatitis C, déi vun der Mamm op d'Kand passéiert sinn, wäerte bis zu 18 Méint präsent sinn, sou datt d'Kanner fir HCV Antikörper net méi fréi wéi dëst getest ginn.
Hepatitis C gëtt entweder vun engem Gastroenterologe, engem Hepatologe (e Gastroenterologe mat zousätzlech Ausbildung an der Lebererkrankheet) oder engem Spezialist fir Infektiounskrankheeten behandelt. D'Behandlungsteam kann méi wéi ee Spezialist enthalen, jee no der Ausmooss vum Leberschued. Chirurgen déi spezialiséiert sinn op Operatioun vun der Liewer, inklusiv Lebertransplantatioun, sinn Deel vum medizinesche Team a solle Patienten mat fortgeschrattem Krankheet gesinn (Leberfehler oder Zirrhose) fréi, ier de Patient eng Liewer Transplantatioun brauch. Si kënne fäeg sinn Themen z'identifizéieren déi musse behandelt ginn ier d'Operatioun berücksichtegt ka ginn. Aner Persounen, déi hëllefräich kënne bei der Gestioun vun Patienten sinn, enthalen Diätetiker fir iwwer Ernärungsprobleemer ze konsultéieren an Apdikter fir mat der Gestioun vun Drogen ze hëllefen.
Et gi verschidde Blutt Tester fir d'Diagnostik vun der Hepatitis C Infektioun. Blutt kann fir Antikörper géint Hepatitis C (Anti-HCV Antikörper) getest ginn. Et dauert ongeféier 8-12 Wochen am Duerchschnëtt, a bis zu 6 Méint, fir Antikörper no der initialer Infektioun mat Hepatitis C z'entwéckelen, sou datt d'Screening fir Antikörper e puer nei infizéiert Individuen vermësst. Antikörper ze hunn ass net eng absolut Indikatioun fir aktiven, multiplizéierend Hepatitis C Virus, awer wann den Antikörpertest positiv ass (Antikörper ass präsent), ass d'statistesch Wahrscheinlechkeet fir eng aktiv Infektioun méi wéi 99%.
Verschidden Tester sinn verfügbar fir d'Quantitéit vum Hepatitis C Virus am Blutt vun enger Persoun ze moossen (viral Belaaschtung). D'RNA vum Hepatitis C Virus kann identifizéiert ginn duerch eng Zort Test genannt Polymerase Kettenreaktioun (PCR), déi zirkuléierend Virus am Blutt esou fréi wéi 2-3 Wochen no der Infektioun erkennt, sou datt et benotzt ka ginn fir verdächtegt akuter Infektioun mat Hepatitis C z'entdecken. fréi Infektioun. Et gëtt och benotzt fir ze bestëmmen ob aktiv Hepatitis bei engem präsent ass deen Antikörper géint Hepatitis C huet, a fir d'viral Belaaschtung während der Behandlung ze verfollegen.
Blutt Tester ginn och gemaach fir d'Genotypen vum HCV z'identifizéieren. Genotypen reagéieren anescht op verschidde Behandlungen, sou datt dës Informatioun wichteg ass bei der Auswiel vum passenden Behandlungsregime.
Schätzung vun der Liewerfibrose mat Hëllef vu Blutttester ass och zimlech zouverlässeg bei der Diagnostik vun klinesch signifikante Narben; Dës enthalen FIB-4, FibroSure, Fibrotest, an Aspartat Aminotransferase-zu-Plaquelet Verhältnis Index (APRI).
De nächste Schrëtt ass den Niveau vun der Liewer Narben ze bestëmmen déi geschitt ass. D'Leberbiopsie erlaabt d'Untersuchung vun enger klenger Probe vu Lebergewebe ënner engem Mikroskop, awer d'Leberbiopsie ass en invasiven Test, an huet bedeitend Risiko vu Blutungen. Et kéint och anormal Beräicher an fréi Krankheet verpassen.
Net-invasiv Tester hunn haaptsächlech d'Leberbiopsie ersat ausser a spezielle Situatiounen. Liver stiffness indicates that advanced liver scarring or cirrhosis may be present. Transient elastography may be used to measure this stiffness by ultrasound or magnetic resonance imaging (MRI).
Pre-treatment evaluation for hepatitis C also should include:
Interferons, for example, Roferon-A and Infergen, and pegylated interferons such as Peg-Intron T , Pegasys, were mainstays of treatment for years. Interferons produced sustained viral response (SVR, or cure) of up to 15%. Later, peglatedll forms produced SVR of 50%-80%. These drugs were injected, had many adverse effects, required frequent monitoring, and were often combined with oral ribavirin, which caused anemia. Treatment durations ranged up to 48 weeks.
Direct-acting anti-viral agents (DAAs) are antiviral drugs that act directly on hepatitis C multiplication.
Hepatitis C treatment is best discussed with a doctor or specialist familiar with current and developing options as this field is changing, and even major guidelines may become outdated quickly.
The latest treatment guidelines by the American Association for the Study of Liver Disease (AASLD) and Infectious Disease Society of America (IDSA) recommends use of DAAs as first-line treatment for hepatitis C infection. The choice of DAA varies by specific virus genotype, and the presence or absence of cirrhosis. In the U.S., specific insurance providers also might influence the choice due to the high cost of DAAs. Although the individual, public health, and cost benefits of treating all patients with hepatitis C is clear, the most difficult barrier to treating all people with HCV is the very high cost of the drug regimens. Patients are encouraged to discuss options with their health care professional.
Treatment is recommended in all patients with chronic hepatitis C unless they have a short life expectancy that is not related to liver disease. Severe life-threatening liver disease may require liver transplantation. Newer therapies with DAAs have allowed more and more patients to be treated.
The ultimate goals of antiviral therapy are to
A side goal is preventing co-infections with other hepatitis viruses, such as A and B, which can cause more liver disease than HCV alone. These can be prevented by vaccines and treatment.
When people first get hepatitis C, the infection is said to be acute. Most people with acute hepatitis C do not have symptoms so they are not recognized as being infected. However, some have low-grade fever, fatigue or other symptoms that lead to an early diagnosis. Others who become infected and have a known exposure to an infected source, such as a needlestick injury, are monitored closely.
Treatment decisions should be made on a case-by-case basis. Response to treatment is higher in acute hepatitis infection than chronic infection. However, many experts prefer to hold off treatment for 8-12 weeks to see whether the patient naturally eliminates the virus without treatment. Approaches to treatment are evolving. Patients with acute hepatitis C infection should discuss treatment options with a health care professional who is experienced in treating the disease. There is no established treatment regimen at this time.
If the hepatitis C RNA remains undetectable at the end of the treatment and follow-up period, this is called a sustained virologic response (SVR) and is considered a cure. Over 90% of people treated with DAAs are cured. These people have significantly reduced liver inflammation, and liver scarring may even be reversed.
About 5% of people who are treated for HCV infection are not cured by some of the older regimens. These people may still have options for cure with the newer regimens.
Few people with hepatitis C are at risk for problems if they are treated, however there are some factors that affect treatment regimens, such as concurrent HIV medications and kidney dysfunction. Some drugs are not safe for people with cirrhosis. Individuals who are unable to comply with the treatment schedule for psychological reasons or ongoing drug or alcohol abuse may not be good candidates for treatment because the drugs are very costly and require adherence to the pill regimen and regular follow-up visits. There are some important drug interactions with some of the medications that should be considered by the health care professional.
People with past hepatitis B or who have chronic active hepatitis B should not be treated for HCV without treating for HBV as well. As highly effective treatment for HCV has emerged, reports of serious hepatitis B have come to light. Similar to HCV, hepatitis B usually does not clear from the liver after acute infection, even though it is far less likely to cause chronic active hepatitis than hepatitis C infection. It remains dormant in most people, but it can reactivate with changes in the immune system. It is not clear why eliminating the HCV can allow the HBV infection to flare up. Hepatitis B screening is an important part of the hepatitis C evaluation. Those who have laboratory evidence of active or past infection with HBV should be monitored while receiving HCV treatment.
Compared to interferons and ribavirin drugs, the side effects of DAAs are far fewer and more tolerable. These side effects usually do not require discontinuation of therapy and are self-limiting after completion of therapy.
Patients with hepatitis B co-infection should be monitored for symptoms of reactivation of hepatitis, which are the same as the symptoms of acute hepatitis. The treating doctor may perform blood screening for this as well.
Hepatitis C is the leading reason for 40% to 45% of liver transplants in the U.S. Hepatitis C usually recurs after transplantation and infects the new liver. Approximately 25% of these patients with recurrent hepatitis will develop cirrhosis within five years of transplantation. Despite this, the five-year survival rate for patients with hepatitis C is similar to that of patients who are transplanted for other types of liver disease.
Most transplant centers delay therapy until recurrent hepatitis C in the transplanted liver is confirmed. Oral, highly effective, direct-acting antivirals have shown encouraging results in patients who have undergone liver transplantation for hepatitis C infection and have recurrent hepatitis C. The choice of therapy needs to be individualized and is rapidly evolving.
Once patients successfully complete treatment, the viral load after treatment determines if there is an SVR or cure. If cure is achieved (undetectable viral load after treatment), no further additional testing is recommended unless the patient has cirrhosis. Those who are not cured will need continued monitoring for progression of liver disease and its complications.
While cure eliminates worsening of fibrosis by hepatitis C, complications may still affect those with cirrhosis. These individuals still need regular screening for liver cancer as well as monitoring for esophageal varices that may bleed.
Because hepatitis B co-infection may reactivate or worsen even after treatment for HCV, monitoring for hepatitis symptoms may be needed after the end of therapy.
At this time there are no effective home or over-the-counter treatments for hepatitis C.
Over several years or decades, chronic inflammation may cause death of liver cells and cirrhosis (scaring, fibrosis). When the liver becomes cirrhotic, it becomes stiff, and it cannot perform its normal functions of clearing waste products from the blood. As fibrosis worsens, symptoms of liver failure begin to appear. This is called "decompensated cirrhosis " or "end-stage liver disease. " Symptoms of end-stage liver disease include:
The liver and spleen have an important function of clearing bacteria from the blood stream. Cirrhosis affects many areas of immune function, including attraction of white blood cells to bacteria, reduced killing of bacteria, reduced production of proteins involved in immune defenses, and decreased life span of white blood cells involved in immune defenses. This may be referred to as having cirrhosis-associated immune dysfunction syndrome or CAIDS.
Transmission of hepatitis C can be prevented in several ways.
Prevention programs aim at needle sharing among drug addicts. Needle exchange programs and education have reduced transmission of hepatitis C infection. However, IV drug users are a difficult to reach population, and rates of hepatitis C remain high among them.
Among health care workers, safe needle-usage techniques have been developed to reduce accidental needlesticks. Newer needle systems prevent manual recapping of needles after use of syringes, which is a frequent cause of accidental needlesticks
There is no clear way to prevent hepatitis C transmission from mother to fetus at this time.
People with multiple sexual partners should use barrier precautions such as condoms to limit the risk of hepatitis C and other sexually transmitted diseases, including HIV.
If one partner is infected, monogamous couples may want to consider the low risk of transmission of hepatitis C infection when deciding whether to use condoms during sex. Some couples may decide to use them and some may not.
Screening of the blood supply has almost eliminated the risk of transmission of hepatitis C infection through transfusion.
People with hepatitis C infection should not share razors or toothbrushes with others because of the possibility that these items may be contaminated with blood.
People who want to get a body piercing(s) or tattoo(s) are encouraged to do so only at licensed piercing and tattoo shops (facilities), and verify that the body piercing or tattoo shop uses infection-control practices.
It is critical that physicians and clinics follow manufacturers and regulatory agency directions for sterilizing/cleaning instruments and that disposable instruments be discarded properly. There is no need to use special isolation procedures when dealing with hepatitis C infected patients.
In general, among patients with untreated hepatitis C:
Drinking alcohol and acquiring other hepatitis viruses are risk factors for worse liver disease. People with chronic hepatitis C should avoid drinking alcohol and should be screened for antibodies to hepatitis A and B. If they do not have antibodies, they should be vaccinated against these other hepatitis viruses.
People with hepatitis C should be educated about preventing HIV infection. Infection with both HIV and hepatitis C speeds up and worsens liver damage caused by hepatitis C. Hepatitis C also can affect the HIV infection and how it is treated. About 25% of people with HIV infection are co-infected (also infected) with hepatitis C, and up to 90% of IV drug users with HIV are co-infected with hepatitis C. Screening for hepatitis viruses is important in all people infected with HIV, just as screening for HIV is important in people who have hepatitis C.
Liver cancer (hepatocellular carcinoma, or hepatoma) is associated with cirrhosis from chronic hepatitis C. Some experts recommend screening patients with hepatitis C infection and cirrhosis for liver cancer periodically.
As our knowledge of hepatitis C increases, more and more patients are being diagnosed with chronic infection. Current research is very active and includes diagnosis, natural history, treatment, and vaccine development. Thus the field is constantly changing, with new guidelines added frequently.
 10 Delicious SIBO Christmas Breakfast Rezepter
10 lecker SIBO Chrëschtfrühstücksrezepter Fänkt de Chrëschtmoien mat engem Knall un mat dëse leckere SIBO Chrëschtfrühstücksrezepter. Si si speziell genuch fir Äre Vakanzefrühstück wäert ze sinn, aw
10 Delicious SIBO Christmas Breakfast Rezepter
10 lecker SIBO Chrëschtfrühstücksrezepter Fänkt de Chrëschtmoien mat engem Knall un mat dëse leckere SIBO Chrëschtfrühstücksrezepter. Si si speziell genuch fir Äre Vakanzefrühstück wäert ze sinn, aw
 Wéi wësse wann Är IBS Pain net Appendicitis ass
A verschiddene Leit kann de Schmerz vum Reizdarmsyndrom (IBS) ganz schwéier sinn a souguer dAppendizis mimikéieren. Si auserneen ze soen ass net sou einfach wéi e puer Leit mengen, a souguer Gesondhee
Wéi wësse wann Är IBS Pain net Appendicitis ass
A verschiddene Leit kann de Schmerz vum Reizdarmsyndrom (IBS) ganz schwéier sinn a souguer dAppendizis mimikéieren. Si auserneen ze soen ass net sou einfach wéi e puer Leit mengen, a souguer Gesondhee
 Naomi vu Milk for the Morning Cake
Mir maachen et eng Prioritéit fir SCD Perséinlechkeeten aus dem ganzen Internet ze markéieren. Mir héiere gär Erfollegsgeschichten a wëllen dWëssen vun deenen, déi daper genuch sinn, verbreeden fir hi
Naomi vu Milk for the Morning Cake
Mir maachen et eng Prioritéit fir SCD Perséinlechkeeten aus dem ganzen Internet ze markéieren. Mir héiere gär Erfollegsgeschichten a wëllen dWëssen vun deenen, déi daper genuch sinn, verbreeden fir hi